

Review
Gastrointestinal complications of obesity surgery
Affiliations
- PMID: 15266241
- PMCID: PMC1395777
Item in Clipboard
Review
Gastrointestinal complications of obesity surgery
MedGenMed.
.
No abstract available
Figures
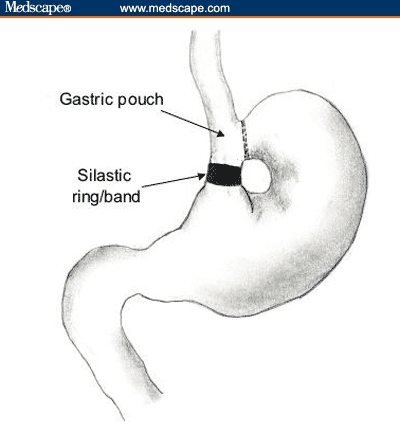
Vertical banded gastroplasty (VBG). A vertical pouch is created by stapling the front of the stomach to the back wall, below the esophagogastric junction. The end of the newly created gastric pouch is constricted with either a 1-cm diameter polypropylene band (VBG) or a 1-cm silastic ring (vertical ring-banded gastroplasty).
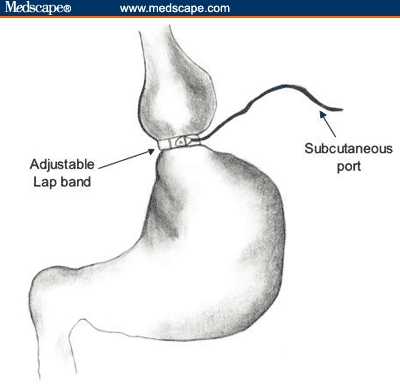
Adjustable laparoscopic banding. A band is laparoscopically placed around the upper stomach to create a restrictive pouch. The balloon in the band is connected to a port that is placed subcutaneously and can be accessed to inflate or deflate the balloon, consequently changing the size of the band circumference.

Roux-en-Y gastric bypass (RYGBP) surgery. A small pouch is created by either stapling or transecting the stomach. The pouch is then connected to and empties into the Roux limb of the jejunum, which is approximately 50–100 cm in length.

(A) Biliopancreatic diversion (BPD) A limited gastrectomy is created, and the transected ileum is anastomosed to the gastric pouch. (B) BPD with duodenal switch. A sleeve gastrectomy is created to maintain the pylorus and avoid anastomotic complications. Similar to classic BPD, the transected, distal small bowel is connected to the stomach via a small part of the first potion of the duodenum.

Anastomotic ulcers: (A) gastric and (B) jejunal or marginal ulcer.

Anastomotic stricture: (A) Gastrografin swallow, (B) anastomotic stricture with a diameter of approximately 5 mm, and (C) dilation with a through-the-scope balloon dilator.
Similar articles
-
Laparoscopic adjustable gastric banding surgery for morbid obesity: imaging of normal anatomic features and postoperative gastrointestinal complications.AJR Am J Roentgenol. 2007 Feb;188(2):472-9. doi: 10.2214/AJR.05.0293. AJR Am J Roentgenol. 2007. PMID: 17242257 Review.
-
[Clinical Practice after Bariatric Surgery: Problems and Complications].Praxis (Bern 1994). 2015 Dec 9;104(25):1379-85. doi: 10.1024/1661-8157/a002204. Praxis (Bern 1994). 2015. PMID: 26649955 Review. German.
-
The role of endoscopy in bariatric surgery.Best Pract Res Clin Gastroenterol. 2008;22(5):839-64. doi: 10.1016/j.bpg.2008.07.002. Best Pract Res Clin Gastroenterol. 2008. PMID: 18790435 Review.
-
[Bariatric surgery and associated complications: radiological imaging].Radiologe. 2011 May;51(5):352-65. doi: 10.1007/s00117-010-2086-6. Radiologe. 2011. PMID: 21512763 Review. German.
-
Gastrointestinal Complications and Management of Obesity.Gastroenterology. 2018 Dec;155(6):1655-1658. doi: 10.1053/j.gastro.2018.08.012. Epub 2018 Aug 10. Gastroenterology. 2018. PMID: 30099075 No abstract available.
Cited by
-
Gastric Emptying and Food Tolerance Following Banded and Non-banded Roux-en-Y Gastric Bypass.Obes Surg. 2019 Feb;29(2):560-568. doi: 10.1007/s11695-018-3561-9. Obes Surg. 2019. PMID: 30402805 Clinical Trial.
-
Effect of Dexmedetomidine Compared to Remifentanil During Bariatric Surgery on Postoperative Nausea and Vomiting: a Retrospective Study.Obes Surg. 2022 Oct;32(10):3368-3374. doi: 10.1007/s11695-022-05894-4. Epub 2022 Aug 17. Obes Surg. 2022. PMID: 35976557
-
Role of Endoscopic Gastroplasty Techniques in the Management of Obesity.Clin Endosc. 2017 Jan;50(1):21-25. doi: 10.5946/ce.2016.147. Epub 2017 Jan 30. Clin Endosc. 2017. PMID: 28147478 Free PMC article. Review.
-
Evaluation of eating habits and lifestyle in patients with obesity before and after bariatric surgery: a single Italian center experience.Springerplus. 2016 Sep 1;5(1):1467. doi: 10.1186/s40064-016-3133-1. eCollection 2016. Springerplus. 2016. PMID: 27652042 Free PMC article.
References
-
- NHANES. National Center on Health Statistics. Results from the 1999-2000 National Health and Nutrition Examination Survey. Prevalence of Overweight and Obesity Among Adults: United States, 1999-2000. Centers for Disease Control October 24, 2002. Available at: http://www.cdc.gov/nchs/products/pubs/pubd/hestats/obese/obse99.htm. Accessed February 1, 2004.
-
- Klein S, Wadden T, Sugerman HJ. AGA technical review on obesity. Gastroenterology. 2002; 123: 882-932. - PubMed
-
- Barrow CJ. Roux-en-Y gastric bypass for morbid obesity. AORN J. 2002; 76: 590, 593-604; quiz 606-608. - PubMed
-
- Pi-Sunyer FX. A review of long-term studies evaluating the efficacy in weight loss ameliorating disorders associated with obesity. Clin Ther. 1996; 18: 1006-1035. - PubMed
-
- Balsiger BM, Murr MM, Poggio JL, Sarr MG. Bariatric surgery. Surgery for weight control in patients with morbid obesity. Med Clin North Am. 2000; 84: 477-489. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical