

Minilaparotomy and endoscopic techniques for tubal sterilisation
- PMID: 15266447
- PMCID: PMC7025802
- DOI: 10.1002/14651858.CD001328.pub2
Minilaparotomy and endoscopic techniques for tubal sterilisation
Abstract
Background: Worldwide, the most commonly used method of fertility regulation is tubal sterilisation. In developed countries sterilisation is generally performed by laparoscopy rather than by minilaparotomy, based on the belief that this approach is both safe and effective. In developing countries, where the resources are limited for the purchase and maintenance of the more sophisticated laparoscopic equipment, minilaparotomy may still be the most common approach. In both resource poor and industrialised countries using the technique with the greatest effectiveness and safety, together with the least costs, is extremely important. Though both methods are widely used, the advantages and disadvantages of laparoscopic sterilisation compared to mini-laparotomy have not been systematically evaluated. The ideal method would be one which is highly effective, economical, able to be performed on an outpatient basis, allowing rapid resumption of normal activity, producing a minimal or invisible scar and having a potential for reversibility. This review considers the methods to enter the abdominal cavity through the abdominal wall, either by minilaparotomy, laparoscopy or culdoscopy regardless of the technique used for tubal sterilisation.
Objectives: To evaluate laparoscopic tubal sterilisation, as compared to minilaparotomy in terms of operative morbidity and mortality. Trials comparing laparoscopy or minilaparotomy with culdoscopy were also included in the review. Different methods used to interrupt tubal patency (excision, occlusion and coagulation) and comparison of different forms of anaesthesia will be considered in different reviews.
Search strategy: Randomised controlled trials (RCTs) have been identified by using the search strategy of the Cochrane Collaboration. The Cochrane Controlled Trials Register was last searched in 1999 (Cochrane Library Issue 4, 1999). Reference lists of identified trials have been searched.
Selection criteria: All randomised controlled trials comparing laparoscopy, minilaparotomy and/or culdoscopy for tubal sterilisation. Except in one trial [Taner 1994] where 4 women underwent curettage at the same time, all women requested tubal sterilisation as an interval procedure.
Data collection and analysis: Trials under consideration were evaluated for methodological quality and appropriateness for inclusion. Data were extracted independently by the reviewers. Results are reported as odds ratio for dichotomous outcomes and weighted mean differences for continuous outcomes.
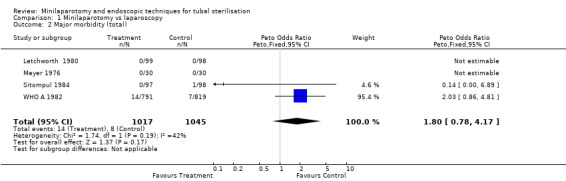
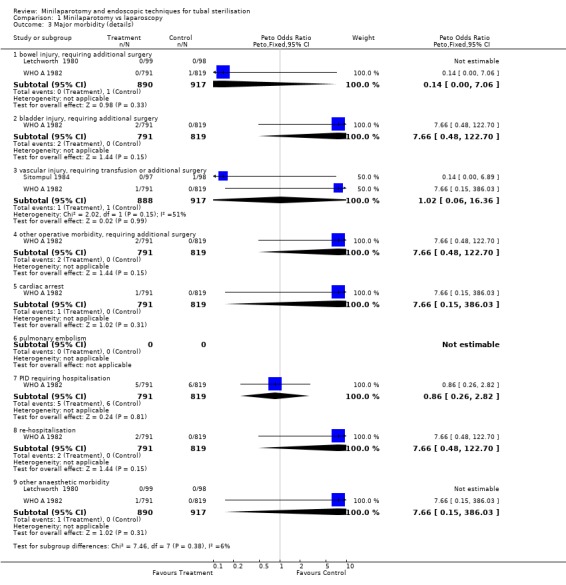
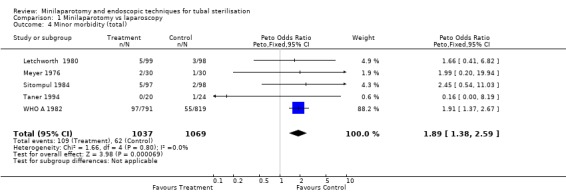
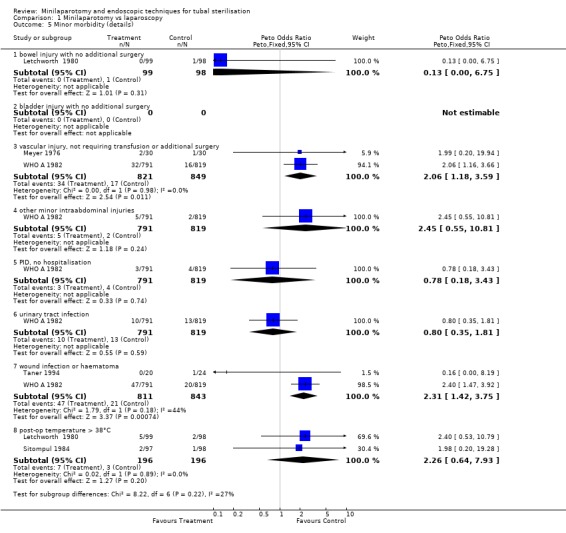
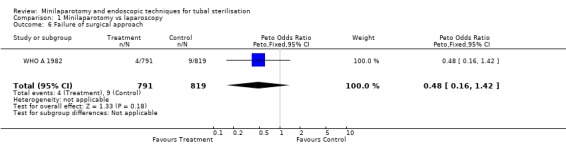
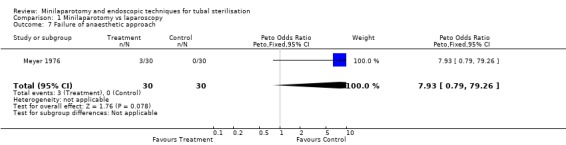
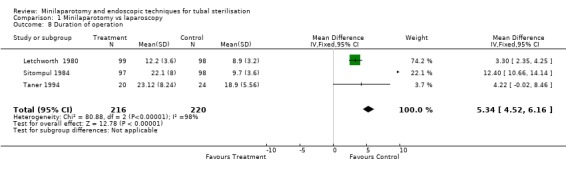
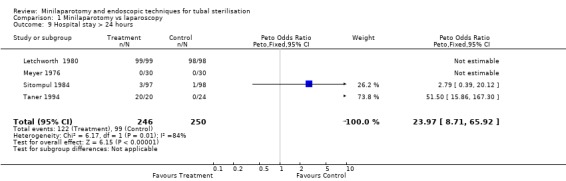
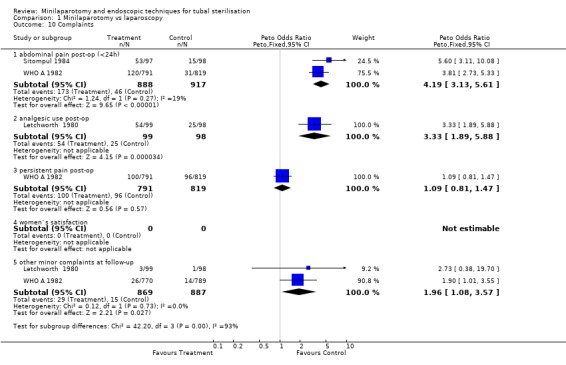
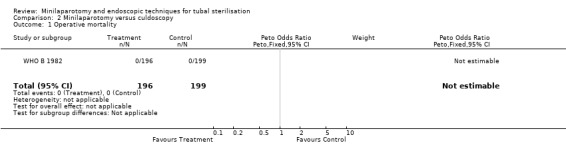
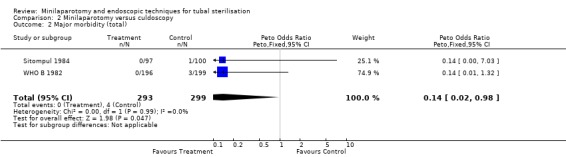
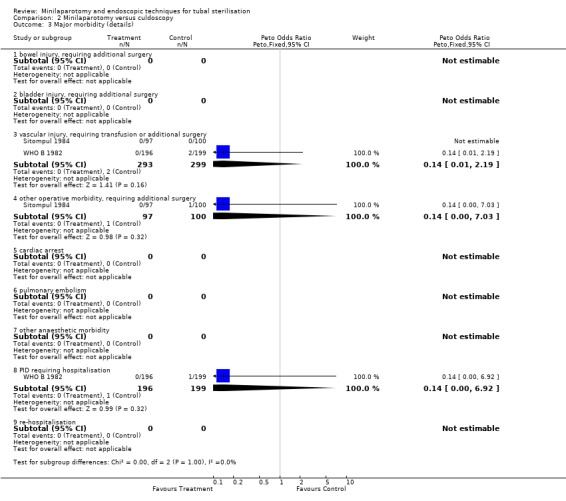
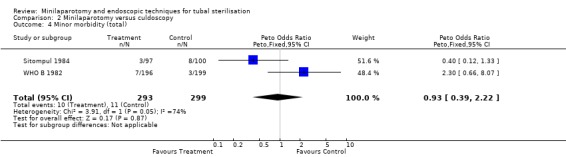
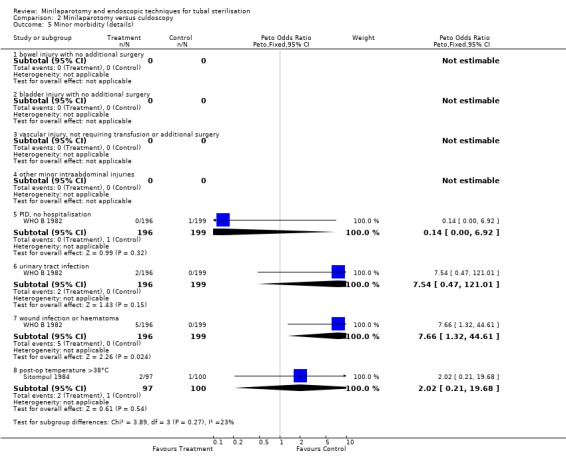
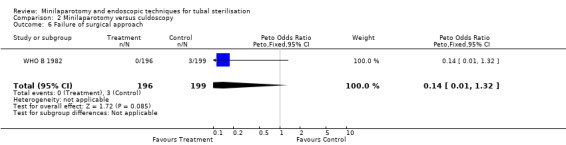
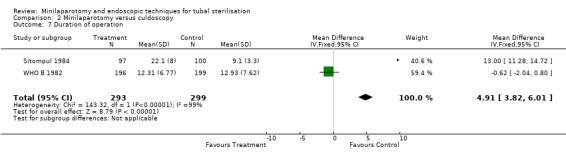
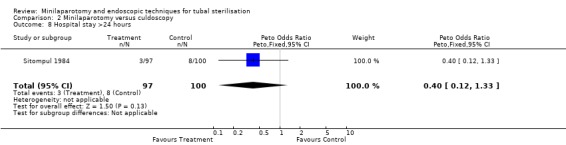
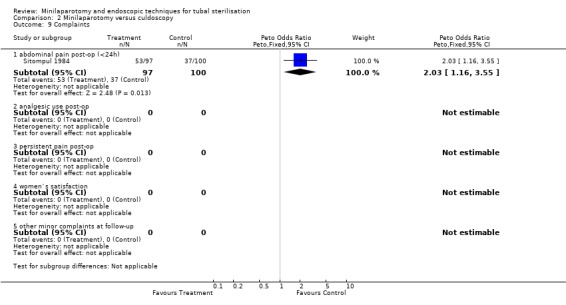
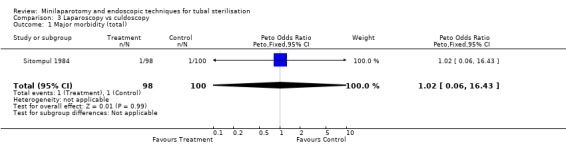
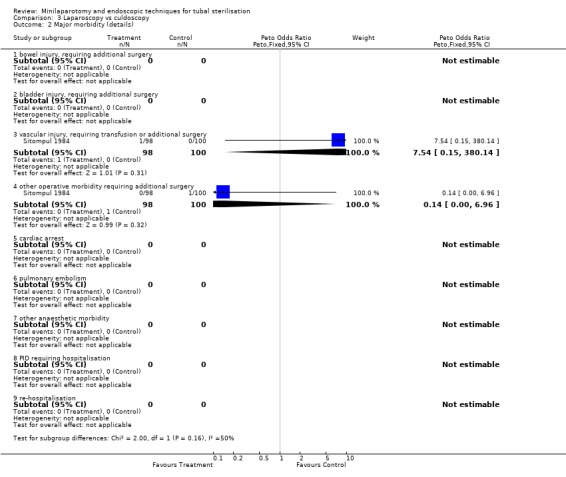
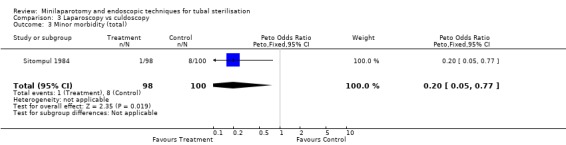
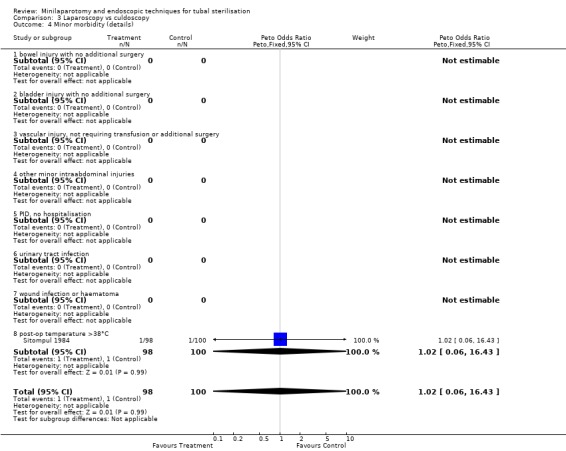
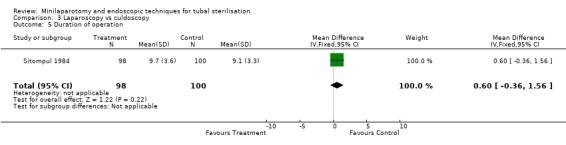
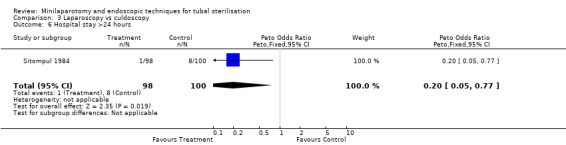
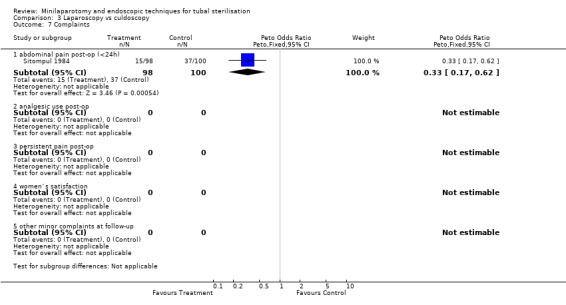
Main results: Minilaparotomy vs laparoscopy: There was no difference in major morbidity between the 2 groups. Minor morbidity was significantly less in the laparoscopy group (Peto OR 1.89; 95% CI 1.38, 2.59). Duration of operation was about 5 minutes shorter in the laparoscopy group (WMD 5.34; 95% CI 4.52, 6.16). Minilaparotomy vs culdoscopy: Women undergoing culdoscopy had more major morbidity than women for whom minilaparotomy was performed (Peto OR 0.14; 95% CI 0.02, 0.98). Duration of operation was about 5 minutes shorter in women undergoing culdoscopy (WMD 4.91; 95% CI 3.82, 6.01). Laparoscopy vs culdoscopy: In the one trial comparing the two interventions there were no significant differences between the groups with regard to major morbidity. Significantly more women suffered from minor morbidities in the culdoscopy group compared to the laparoscopy group (Peto OR 0.20; 95% CI 0.05, 0.77).
Reviewers' conclusions: Major morbidity seems to be a rare outcome for both, laparoscopy and minilaparotomy. The included studies had limited power to demonstrate significant differences especially for the relatively rare but potentially serious outcomes. Personal preference of the woman and/or of the surgeon can guide the choice of technique. Practical aspects (e.g. cost, maintenance, and sterilisation of the instruments) must be taken into account before implementing the more sophisticated endoscopic techniques in settings with limited resources. Culdoscopy is not recommended as it carries a higher complication rate.
Conflict of interest statement
None
Figures
Update of
-
Minilaparotomy and endoscopic techniques for tubal sterilisation.Cochrane Database Syst Rev. 2002;(3):CD001328. doi: 10.1002/14651858.CD001328. Cochrane Database Syst Rev. 2002. Update in: Cochrane Database Syst Rev. 2004;(3):CD001328. doi: 10.1002/14651858.CD001328.pub2. PMID: 12137624 Updated.
References
References to studies included in this review
Letchworth 1980 {published data only}
-
- Letchworth AT, Kane JL, Noble AD. Laparoscopy or laparotomy for sterilization of women. Obstet Gynecol 1980;56(1):119‐121. - PubMed
Meyer 1976 {published data only}
-
- Meyer JH, King TM. Advances in Female Sterilisation Techniques. Hagerstown, Maryland, 1976. journal 1976;1:Advances in Female Sterilisation Techniques. Hagerstown, Maryland, 1976. Harper & Row, Publishers.
Sitompul 1984 {published data only}
-
- Sitompul H, Lun KC, Lumbanraja M, Kaban RM, Albar E, Simanjuntak P, Hanafiah MJ. Comparison of three types of tubal sterilisation: the Medan experience. Contraception 1984;29(1):55‐63. - PubMed
Taner 1994 {published data only}
-
- Taner CE, Aban M, Yilmaz N, Senturk N, Toy E. Pomeroy tubal ligation by laparoscopy and minilaparotomy. Adv Contracep 1994;10:151‐155. - PubMed
WHO A 1982 {published data only}
-
- World Health Organization, Task Force on Female Sterilization, Special programme of Research, Development and Research Training in Human Reproduction. Minilaparotomy or laparoscopy for sterilization. Am J Obstet Gynecol 1982;143:645‐652. - PubMed
WHO B 1982 {published data only}
-
- World Health Organization. Task Force on Female Sterilization, Special Programme of Research, Development and Research Training in Human Reproduction. Randomized comparative study of culdoscopy and minilaparotomy for surgical contraception in women. Contraception 1982;26(6):587‐593. - PubMed
References to studies excluded from this review
Sherman 1984 {published data only}
-
- Sherman PA, Burigo JA. Comparison of laparoscopic Falope‐ring and minilaparotomy sterilization. Obstetrics & Gynecology 1984;63:71‐74. - PubMed
Tiras 2000 {published data only}
-
- Tiras MB, Noyan V, Gokce O, Guner H, Yildirim M, Risquez F. Comparison of microlaparoscopy for tubal sterilization under local anaesthesia with mild sedation: a prospective randomzed study. Fertility 2000. - PubMed
Additional references
Destefano 1983
-
- Destefano F, Greenspan JR, Dicker RC, Peterson HB, et al. Complications of interval laparoscopic tubal sterilisation. journal 1983;61:153‐158. - PubMed
Franks 1987
-
- Franks AL, Kendrick JS, Peterson HB. Unintended laparotomy associated with laparoscopic tubal sterilization. American Journal of Obstetrics and Gynecology 1987;157:1102‐1105. - PubMed
Hillis 1998
-
- Hillis SD, Marchbanks PA, Taylor LR, Peterson HB. Higher hysterectomy risk for sterilized than nonsterilized women: findings from the US Collaborative Review of Sterilization. The US Collaborative Review of Sterilization Working Group. Obstetrics Gynecology 1998;91:241‐246. - PubMed
Limpaphayom 1991
-
- Limpaphayom K. Sterilization. Curr Opin Obstet Gynecol 1991;3:501‐509. - PubMed
Osathanondh 1974
-
- Osathanondh V. Suprapubic mini‐laparotomy, uterine elevation technique: simple, inexpensive and out‐patient procedure for interval female sterilization. Contraception 1974;10:251‐262. - PubMed
Uchida 1975
-
- Uchida H. Uchida tubal sterilization. Am J Obstet Gynecol 1975;121:153‐158. - PubMed
Wheeless 1972
-
- Wheeless CR. Outpatient laparoscope sterilization under local anesthesia. Obstet Gynecol 1972;39:767‐770. - PubMed
Wheeless 1992
-
- Wheeless CR Jr. Tubal sterilization. In: Te Linde's Operative gynecology. [Tubal sterilization]. In: Thompson JD, Rock JA editor(s). Book. Vol. 1, Philadelphia: JB Lippincott, 1992:343‐59.
WHO 1992
-
- World Health Organization. Female sterilization: a guide to provision of services. journal 1992;1:a guide to provision of services. WHO, Geneva, 1992.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical