

Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey
- PMID: 15273542
- PMCID: PMC1360123
- DOI: 10.1097/01.sla.0000133083.54934.ae
Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey
Abstract
Objective: Although quality assessment is gaining increasing attention, there is still no consensus on how to define and grade postoperative complications. This shortcoming hampers comparison of outcome data among different centers and therapies and over time.
Patients and methods: A classification of complications published by one of the authors in 1992 was critically re-evaluated and modified to increase its accuracy and its acceptability in the surgical community. Modifications mainly focused on the manner of reporting life-threatening and permanently disabling complications. The new grading system still mostly relies on the therapy used to treat the complication. The classification was tested in a cohort of 6336 patients who underwent elective general surgery at our institution. The reproducibility and personal judgment of the classification were evaluated through an international survey with 2 questionnaires sent to 10 surgical centers worldwide.
Results: The new ranking system significantly correlated with complexity of surgery (P < 0.0001) as well as with the length of the hospital stay (P < 0.0001). A total of 144 surgeons from 10 different centers around the world and at different levels of training returned the survey. Ninety percent of the case presentations were correctly graded. The classification was considered to be simple (92% of the respondents), reproducible (91%), logical (92%), useful (90%), and comprehensive (89%). The answers of both questionnaires were not dependent on the origin of the reply and the level of training of the surgeons.
Conclusions: The new complication classification appears reliable and may represent a compelling tool for quality assessment in surgery in all parts of the world.
Figures
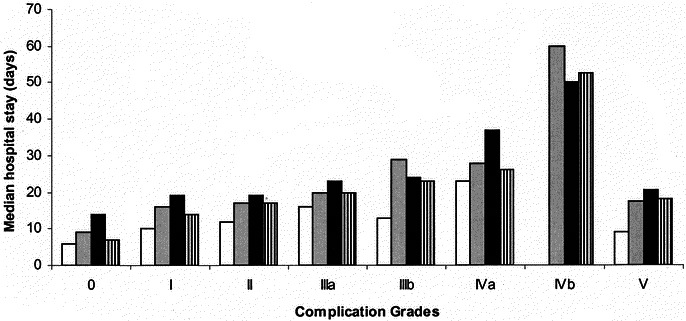
 ), Operation Type B; (▪), Operation Type C; (▥), overall.
), Operation Type B; (▪), Operation Type C; (▥), overall.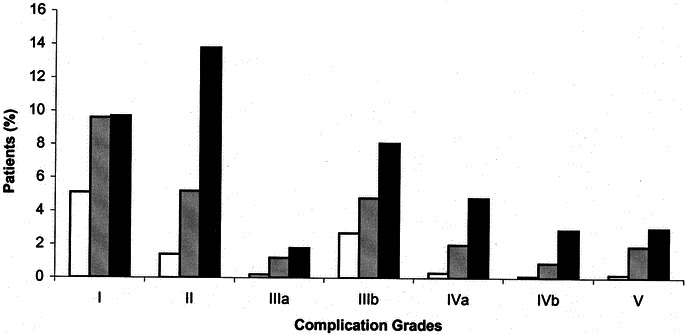 ) < Operation Type C (▪).
) < Operation Type C (▪).Comment in
-
Measuring morbidity.Ann Surg. 2004 Aug;240(2):214-5. doi: 10.1097/01.sla.0000133124.62619.1f. Ann Surg. 2004. PMID: 15273543 Free PMC article. No abstract available.
References
-
- Clavien P, Sanabria J, Strasberg S. Proposed classification of complication of surgery with examples of utility in cholecystectomy. Surgery. 1992;111:518–526. - PubMed
-
- Khuri SF, Daley J, Henderson W. et al.The Department of Veterans Affairs’ NSQIP: the first national, validated, outcome-based, risk-adjusted, and peer-controlled program for the measurement and enhancement of the quality of surgical care. National VA Surgical Quality Improvement Program. Ann Surg. 1998;228:491–507. - PMC - PubMed
-
- Nashef SA, Roques F, Michel P. et al.European system for cardiac operative risk evaluation (EuroSCORE). Eur J Cardiothorac Surg. 1999;16:9–13. - PubMed
-
- Daley J, Henderson W, Khuri S. Risk-adjusted surgical outcomes. Annu Rev Med. 2001;52:275–287. - PubMed
-
- Pomposelli J, Gupta S, Zacharoulis D. et al.Surgical complication outcome (SCOUT) score: a new method to evaluate quality of care in vascular surgery. J Vasc Surg. 1997;25:1007–1015. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
