

Salvage surgery following downstaging of unresectable hepatocellular carcinoma
- PMID: 15273555
- PMCID: PMC1356407
- DOI: 10.1097/01.sla.0000133123.11932.19
Salvage surgery following downstaging of unresectable hepatocellular carcinoma
Abstract
Objective: We reported here a series of 49 patients with unresectable hepatocellular carcinoma (HCC) who underwent nonsurgical treatment to downstage the disease followed by salvage surgery, their long-term outcome, and pattern of recurrence.
Summary background data: Most HCC patients present with unresectable disease and are treated with chemotherapy or intra-arterial therapy with a palliative intent. Occasionally, there are good responses to treatment so that salvage surgery becomes feasible afterward. However, long-term outcomes of these patients are seldom reported.
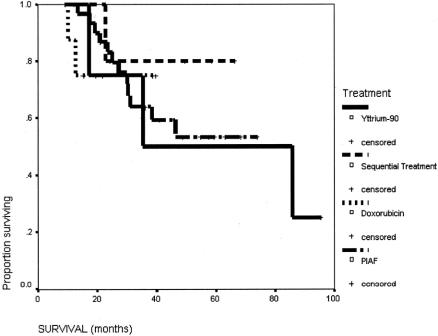
Methods: Patients with unresectable hepatocellular carcinoma, from September 1993 to June 2002, who received salvage surgery after downstaging by systemic chemotherapy, intra-arterial yttrium-90 microspheres, or sequential treatment were included in this study. Systemic chemotherapy consisted of combination doxorubicin, cisplatin, interferon-alpha and 5-fluorouracil (5-FU), or single-agent doxorubicin. The choice of treatment was according to stage of disease and contemporary clinical trial protocol. Survival, recurrence pattern, and surgical outcome were studied.
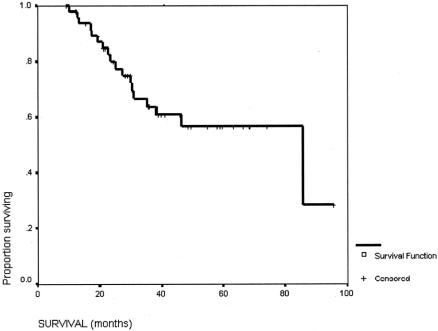
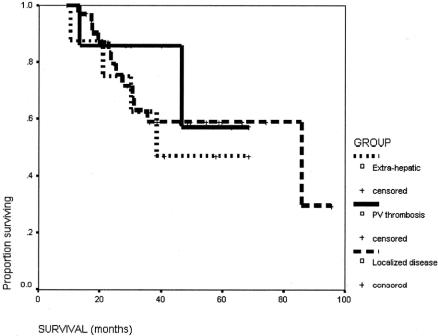
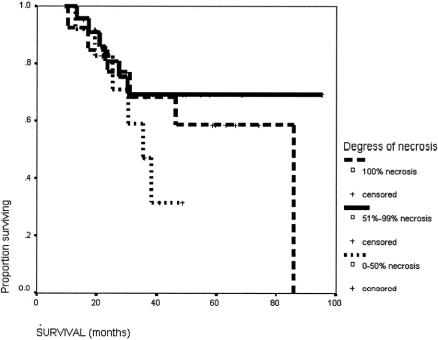
Results: There were 49 patients in this study with 40 males and 9 females, age ranged from 12 to 69 years. Forty patients (81.6%) were hepatitis B positive. Thirty-two patients had combination chemotherapy alone (65.3%), 8 patients had single agent chemotherapy alone (16.3%), 4 patients received intra-arterial yttrium-90 microspheres alone (8.2%), and 5 patients received sequential therapy (10.2%). Twenty-eight (57.1%) patients received major hepatic resection. Thirteen patients (26.5%) had complete necrosis of the tumor after treatment. Twenty-one patients (42.9%) had recurrence after surgery, and 14 of them were intrahepatic recurrence. The median survival was 85.9 months. The 1-year, 3-year, and 5-year survival rates were 98%, 64%, and 57%, respectively.
Conclusions: Salvage surgery after successful downstaging can provide long-term control of disease in a small proportion of patients with unresectable hepatocellular carcinoma.
Figures
References
-
- Lau WY. Management of hepatocellular carcinoma. J R Coll Surg Edinb. 2002;47:389–399. - PubMed
-
- Fan J, Tang ZY, Yu YQ, et al. Improved survival with resection after transcatheter arterial chemoembolisation (TACE) for unresectable hepatocellular carcinoma. Dig Surg. 1998;15:674–678. - PubMed
-
- Tang ZY, Yu YQ, Zhou XD, et al. Cytoreduction and sequential resection for surgically verified unresectable hepatocellular carcinoma: evaluation with analysis of 72 patients. World J Surg. 1995;19:784–789. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
