

Small B cell lymphocytic lymphoma presenting as obstructive sleep apnea
- PMID: 15282026
- PMCID: PMC509285
- DOI: 10.1186/1477-7819-2-26
Small B cell lymphocytic lymphoma presenting as obstructive sleep apnea
Abstract
Background: Most lymphomas that involve the tonsil are large B cell lymphomas. Large B-cell lymphoma is a high grade malignancy which progresses rapidly. Tonsillar lymphoma usually presents as either a unilaterally enlarged palatine tonsil or as an ulcerative and fungating lesion over the tonsillar area. Small lymphocytic lymphomas (SLL) of the Waldeyer's ring are uncommon.
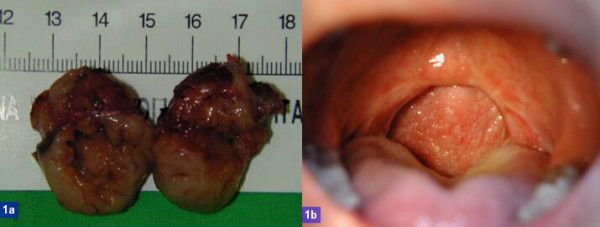
Case presentation: We report a 41-year-old male who presented with a ten-year history of snoring. Physical examination revealed smooth bilateral symmetrically enlarged tonsils without abnormal surface change or cervical lymphadenopathy. Palatal redundancy and a narrowed oropharyngeal airway were also noted. The respiratory disturbance index (RDI) was 66 per hour, and severe obstruction sleep apnea (OSA) was suspected. No B symptoms, sore throat, odynophagia or dysphagia was found. We performed uvulopalatopharyngoplasty (UPPP) and pathological examination revealed incidental small B-cell lymphocytic lymphoma (SLL).
Conclusion: It is uncommon for lymphoma to initially present as OSA. SLL is an indolent malignancy and is not easy to detect in the early stage. We conclude that SLL may be a contributing factor of OSA in the present case.
Figures


Similar articles
-
Bilateral Tonsillar Enlargement as a First Manifestation of Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma with an Unusual Interfollicular Pattern of Infiltration.Indian J Hematol Blood Transfus. 2016 Jun;32(Suppl 1):152-5. doi: 10.1007/s12288-015-0629-8. Epub 2015 Dec 11. Indian J Hematol Blood Transfus. 2016. PMID: 27408379 Free PMC article.
-
[Bilateral tonsillar hypertrophy as the first manifestation of B cell-small lymphocytic lymphoma with interfolicular pattern].Rev Med Inst Mex Seguro Soc. 2010 Jan-Feb;48(1):75-8. Rev Med Inst Mex Seguro Soc. 2010. PMID: 20696111 Spanish.
-
Unilateral Tonsillar Enlargement as Initial Presentation of Bilateral Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma.Ear Nose Throat J. 2023 Nov 24:1455613231214634. doi: 10.1177/01455613231214634. Online ahead of print. Ear Nose Throat J. 2023. PMID: 37997620
-
Surgical treatment of snoring & obstructive sleep apnoea.Indian J Med Res. 2010 Feb;131:267-76. Indian J Med Res. 2010. PMID: 20308752 Review.
-
Waldeyer's ring lymphoma presenting as massive oropharyngeal hemorrhage.Mo Med. 2000 Feb;97(2):63-5. Mo Med. 2000. PMID: 10731755 Review.
Cited by
-
Bilateral Tonsillar Enlargement as a First Manifestation of Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma with an Unusual Interfollicular Pattern of Infiltration.Indian J Hematol Blood Transfus. 2016 Jun;32(Suppl 1):152-5. doi: 10.1007/s12288-015-0629-8. Epub 2015 Dec 11. Indian J Hematol Blood Transfus. 2016. PMID: 27408379 Free PMC article.
-
Covid-19 and Obstructive Sleep Apnea: The Theatricals and Quality-of-Life Impact.Indian J Otolaryngol Head Neck Surg. 2023 Apr 19;75(3):1-11. doi: 10.1007/s12070-023-03730-4. Online ahead of print. Indian J Otolaryngol Head Neck Surg. 2023. PMID: 37362137 Free PMC article.
-
Sleep disruption in hematopoietic cell transplantation recipients: prevalence, severity, and clinical management.Biol Blood Marrow Transplant. 2014 Oct;20(10):1465-84. doi: 10.1016/j.bbmt.2014.04.010. Epub 2014 Apr 18. Biol Blood Marrow Transplant. 2014. PMID: 24747335 Free PMC article. Review.
-
Deep cervical lymph node hypertrophy: a new paradigm in the understanding of pediatric obstructive sleep apnea.Laryngoscope. 2013 Aug;123(8):2043-9. doi: 10.1002/lary.23748. Epub 2013 May 10. Laryngoscope. 2013. PMID: 23666635 Free PMC article.
-
Obstructive sleep apnea syndrome caused by uncommon tumors of the upper aerodigestive tract.Int J Clin Exp Pathol. 2014 Sep 15;7(10):6686-93. eCollection 2014. Int J Clin Exp Pathol. 2014. PMID: 25400748 Free PMC article.
References
-
- Arens R, McDonough JM, Costarino AT, Mahboubi S, Tayag-Kier CE, Maislin G, Schwab RJ, Pack AI. Magnetic resonance imaging of the upper airway structure of children with obstructive sleep apnea syndrome. Am J Respir Crit Care Med. 2001;164:698–703. - PubMed
-
- Strohl KP. Obstructive sleep apnea-hypopnea syndrome. In: Goldman L, Ausiello D, editor. Cecil Textbook of Medicine. Philadelphia, W.B. Saunders Company; 2000. pp. 462–426.
-
- Keating MJ. Chronic lymphocytic leukemia. In: Goldman L, Ausiello D, editor. Cecil Textbook of Medicine. Philadelphia, W.B. Saunders Company; 2000. pp. 949–953.
-
- Nolan P. Chronic lymphatic leukemia presenting as severe obstructive sleep apnea. Respirology. 1996;1:299–301. - PubMed
-
- Zorick F, Roth T, Kramer M, Flessa H. Exacerbation of upper-airway sleep apnea by lymphocytic lymphoma. Chest. 1980;77:689–690. - PubMed
LinkOut - more resources
Full Text Sources
