

Impaired gallbladder motility and delayed orocecal transit contribute to pigment gallstone and biliary sludge formation in beta-thalassemia major adults
- PMID: 15285024
- PMCID: PMC4576293
- DOI: 10.3748/wjg.v10.i16.2383
Impaired gallbladder motility and delayed orocecal transit contribute to pigment gallstone and biliary sludge formation in beta-thalassemia major adults
Abstract
Aim: Gallbladder and gastrointestinal motility defects exist in gallstones patients and to a lesser extent in pigment gallstone patients. To investigated the role of gallbladder and gastrointestinal motility disorders in pigment gallstone formation in beta-thalassemia major.
Methods: Twenty-three patients with beta-thalassemia major (16 females; age range 18-37 years) and 70 controls (47 females, age range 18-40 years) were studied for gallbladder and gastric emptying (functional ultrasonography), orocecal transit (OCTT, H(2)-breath test), autonomic dysfunction (sweat-spot, cardiorespiratory reflex tests), bowel habits, gastrointestinal symptoms and quality of life (all with questionnaires). Gallbladder content (ultrasonography) was examined before and during 8-12 mo follow-up.
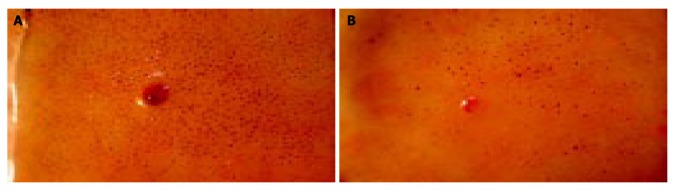
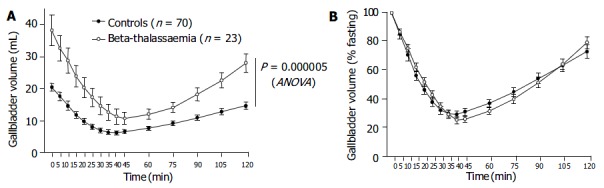
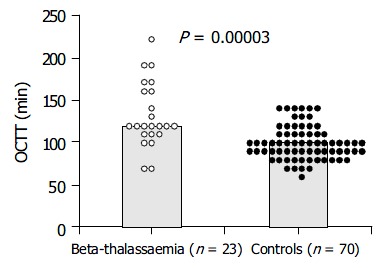
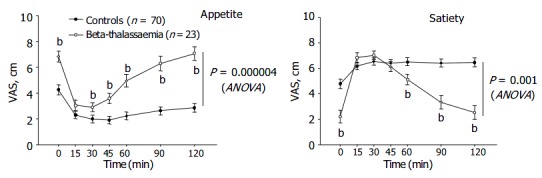
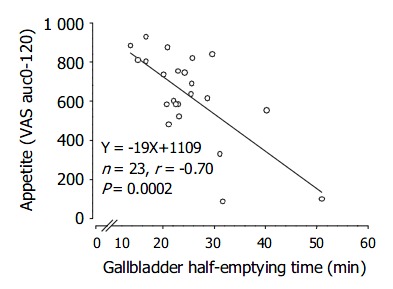
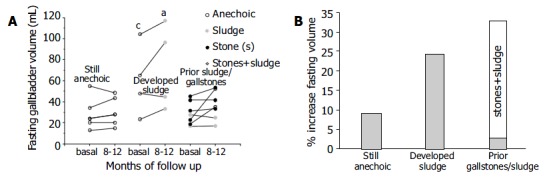
Results: Gallstones and/or biliary sludge were found in 13 (56%) patients. beta-thalassemia major patients had increased fasting (38.0+/-4.8 mL vs 20.3+/-0.7 mL, P = 0.0001) and residual (7.9+/-1.3 mL vs 5.1+/-0.3 mL, P = 0.002) volume and slightly slower emptying (24.9+/-1.7 min vs 20.1+/-0.7 min, P = 0.04) of the gallbladder, together with longer OCTT (132.2+/-7.8 min vs 99.7+/-2.3 min, P = 0.00003) than controls. No differences in gastric emptying and bowel habits were found. Also, patients had higher dyspepsia (score: 6.7+/-1.2 vs 4.9+/-0.2, P = 0.027), greater appetite (P = 0.000004) and lower health perception (P = 0.00002) than controls. Autonomic dysfunction was diagnosed in 52% of patients (positive tests: 76.2% and 66.7% for parasympathetic and sympathetic involvement, respectively). Patients developing sludge during follow-up (38%, 2 with prior stones) had increased fasting and residual gallbladder volume.
Conclusion: Adult beta-thalassemia major patients have gallbladder dysmotility associated with delayed small intestinal transit and autonomic dysfunction. These abnormalities apparently contribute together with haemolytic hyperbilirubinemia to the pathogenesis of pigment gallstones/sludge in beta-thalassemia major.
Figures
Similar articles
-
Gastrointestinal defects in gallstone and cholecystectomized patients.Eur J Clin Invest. 2019 Mar;49(3):e13066. doi: 10.1111/eci.13066. Epub 2019 Jan 29. Eur J Clin Invest. 2019. PMID: 30592298 Free PMC article.
-
Slow-transit constipation: solitary symptom of a systemic gastrointestinal disease.Dis Colon Rectum. 1999 Feb;42(2):231-40. doi: 10.1007/BF02237134. Dis Colon Rectum. 1999. PMID: 10211501
-
Sluggish small bowel motility is involved in determining increased biliary deoxycholic acid in cholesterol gallstone patients.Am J Gastroenterol. 1999 Sep;94(9):2453-9. doi: 10.1111/j.1572-0241.1999.01375.x. Am J Gastroenterol. 1999. PMID: 10484008
-
Update on the Molecular Mechanisms Underlying the Effect of Cholecystokinin and Cholecystokinin-1 Receptor on the Formation of Cholesterol Gallstones.Curr Med Chem. 2019;26(19):3407-3423. doi: 10.2174/0929867324666170619104801. Curr Med Chem. 2019. PMID: 28625150 Free PMC article. Review.
-
Coordinate regulation of gallbladder motor function in the gut-liver axis.Hepatology. 2008 Jun;47(6):2112-26. doi: 10.1002/hep.22204. Hepatology. 2008. PMID: 18506897 Review.
Cited by
-
Gastrointestinal symptoms and motility disorders in patients with systemic scleroderma.BMC Gastroenterol. 2008 Feb 27;8:7. doi: 10.1186/1471-230X-8-7. BMC Gastroenterol. 2008. PMID: 18304354 Free PMC article.
-
Ultrasonographic assessment of gastric and gallbladder dynamics in human health and disease.Intern Emerg Med. 2025 Jun;20(4):965-983. doi: 10.1007/s11739-025-03905-7. Epub 2025 Feb 27. Intern Emerg Med. 2025. PMID: 40016490 Review.
-
Subclinical autonomic dysfunction in patients with β-thalassemia.Clin Auton Res. 2012 Jun;22(3):147-50. doi: 10.1007/s10286-011-0154-2. Epub 2011 Dec 15. Clin Auton Res. 2012. PMID: 22170296
-
Cholecystectomy and risk of metabolic syndrome.Eur J Intern Med. 2018 Jul;53:3-11. doi: 10.1016/j.ejim.2018.04.019. Epub 2018 Apr 26. Eur J Intern Med. 2018. PMID: 29706426 Free PMC article. Review.
-
Gallbladder function predicts subsequent biliary complications in patients with common bile duct stones after endoscopic treatment?BMC Gastroenterol. 2018 Feb 27;18(1):32. doi: 10.1186/s12876-018-0762-6. BMC Gastroenterol. 2018. PMID: 29486713 Free PMC article.
References
-
- Portincasa P, Di Ciaula A, Baldassarre G, Palmieri V, Gentile A, Cimmino A, Palasciano G. Gallbladder motor function in gallstone patients: sonographic and in vitro studies on the role of gallstones, smooth muscle function and gallbladder wall inflammation. J Hepatol. 1994;21:430–440. - PubMed
-
- Portincasa P, Di Ciaula A, Vendemiale G, Palmieri V, Moschetta A, Vanberge-Henegouwen GP, Palasciano G. Gallbladder motility and cholesterol crystallization in bile from patients with pigment and cholesterol gallstones. Eur J Clin Invest. 2000;30:317–324. - PubMed
-
- Portincasa P, Di Ciaula A, Palmieri V, Velardi A, VanBerge-Henegouwen GP, Palasciano G. Impaired gallbladder and gastric motility and pathological gastro-oesophageal reflux in gallstone patients. Eur J Clin Invest. 1997;27:653–661. - PubMed
-
- Rodgers GP. Hemogloblinopathies: The Thalassemias. In: Goldmann L, Bennett JC, editors. Cecil. Textbook of Medicine. Philadelphia: W.B. Saunders Company. 2000
MeSH terms
LinkOut - more resources
Full Text Sources
