

Stress echocardiography in heart failure
- PMID: 15285780
- PMCID: PMC514499
- DOI: 10.1186/1476-7120-2-11
Stress echocardiography in heart failure
Abstract
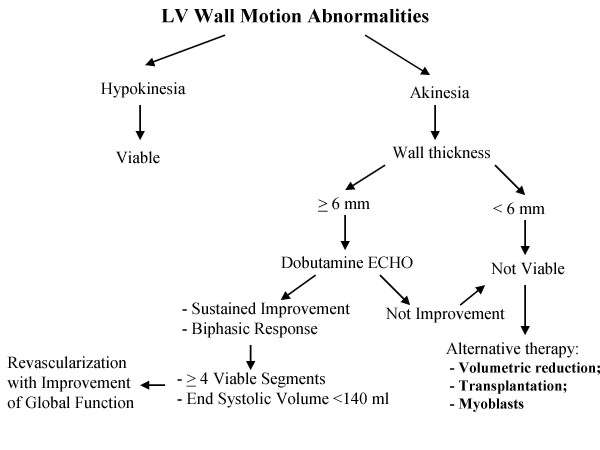
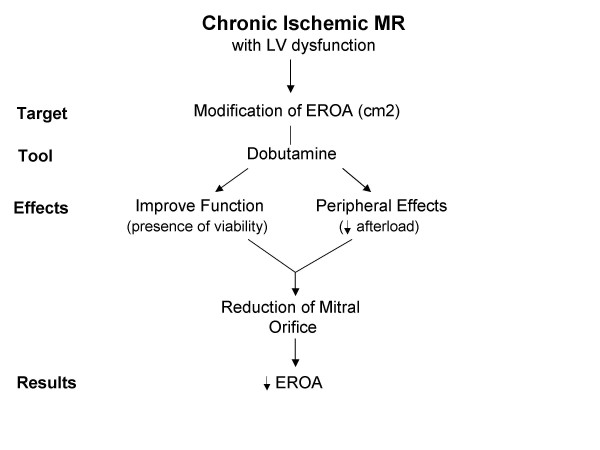
Echocardiography has the ability to noninvasively explore hemodynamic variables during pharmacologic or exercise stress test in patients with heart failure. In this review, we detail some important potential applications of stress echocardiography in patients with heart failure. In patients with coronary artery disease and chronic LV dysfunction, dobutamine stress echocardiography is able to distinguish between viable and fibrotic tissue to make adequate clinical decisions. Exercise testing, in combination with echocardiographic monitoring, is a method of obtaining accurate information in the assessment of functional capacity and prognosis. Functional mitral regurgitation is a common finding in patients with dilated and ischaemic cardiomyopathy and stress echocardiography in the form of exercise or pharmacologic protocols can be useful to evaluate the behaviour of mitral regurgitation. It is clinical useful to search the presence of contractile reserve in non ischemic dilated cardiomyopathy such as to screen or monitor the presence of latent myocardial dysfunction in patients who had exposure to cardiotoxic agents. Moreover, in patients with suspected diastolic heart failure and normal systolic function, exercise echocardiography could be able to demonstrate the existence of such dysfunction and determine that it is sufficient to limit exercise tolerance. Finally, in the aortic stenosis dobutamine echocardiography can distinguish severe from non-severe stenosis in patients with low transvalvular gradients and depressed left ventricular function.
Figures







Similar articles
-
Clinical aspects of left ventricular diastolic function assessed by Doppler echocardiography following acute myocardial infarction.Dan Med Bull. 2001 Nov;48(4):199-210. Dan Med Bull. 2001. PMID: 11767125 Review.
-
Enoximone echocardiography: a novel test to evaluate left ventricular contractile reserve in patients with heart failure on chronic beta-blocker therapy.Cardiovasc Ultrasound. 2003 Sep 25;1:13. doi: 10.1186/1476-7120-1-13. Cardiovasc Ultrasound. 2003. PMID: 14596683 Free PMC article. Clinical Trial.
-
[Contribution of echocardiography to the diagnosis of patients with chronic heart failure].Ital Heart J Suppl. 2000 Oct;1(10):1311-6. Ital Heart J Suppl. 2000. PMID: 11068713 Review. Italian.
-
[Echocardiography in aortic stenosis: new insights into challenging scenarios].Ital Heart J Suppl. 2004 Jun;5(6):457-65. Ital Heart J Suppl. 2004. PMID: 15471150 Review. Italian.
-
Low-level exercise echocardiography fails to elicit left ventricular contractile reserve in patients with aortic stenosis, reduced ejection fraction, and low transvalvular gradient.Echocardiography. 2007 Jan;24(1):47-51. doi: 10.1111/j.1540-8175.2007.00349.x. Echocardiography. 2007. PMID: 17214622
Cited by
-
Prognostic importance of tissue velocity imaging during exercise echocardiography in patients with systolic heart failure.Echo Res Pract. 2015 Mar 1;2(1):19-27. doi: 10.1530/ERP-14-0074. Epub 2015 Mar 3. Echo Res Pract. 2015. PMID: 26693312 Free PMC article.
-
Cardiopulmonary exercise testing and echocardiographic exam: an useful interaction.Cardiovasc Ultrasound. 2019 Dec 3;17(1):29. doi: 10.1186/s12947-019-0180-0. Cardiovasc Ultrasound. 2019. PMID: 31796047 Free PMC article. Review.
-
Exercise stress echocardiography: Where are we now?World J Cardiol. 2022 Feb 26;14(2):64-82. doi: 10.4330/wjc.v14.i2.64. World J Cardiol. 2022. PMID: 35316975 Free PMC article. Review.
-
Presence of left ventricular contractile reserve, evaluated by means of dobutamine stress-echo test, is able to predict response to cardiac resynchronization therapy.J Interv Card Electrophysiol. 2008 Nov;23(2):121-6. doi: 10.1007/s10840-008-9255-9. Epub 2008 Jun 28. J Interv Card Electrophysiol. 2008. PMID: 18587637
-
Role of echocardiography in diagnosis and risk stratification in heart failure with left ventricular systolic dysfunction.Cardiovasc Ultrasound. 2007 Oct 2;5:34. doi: 10.1186/1476-7120-5-34. Cardiovasc Ultrasound. 2007. PMID: 17910744 Free PMC article. Review.
References
-
- Shulz R, Heusch G. Characterization of hibernating and stunned myocardium. Eur Heart J. 1995;16:19–25. - PubMed
-
- Braunwald E, Kloner RA. The stunned myocardium: prolonged, postischemic ventricular dysfunction. Circulation. 1982;66:1146–1149. - PubMed
-
- Kloner RA, Bolli R, Marban E, Reinlib L, Braunwald E. Medical and cellular implications of stunning, hibernation, and preconditioning: an NHLBI workshop. Circulation. 1998;97:1848–1867. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
