

Vitamin B12 (cobalamin) deficiency in elderly patients
- PMID: 15289425
- PMCID: PMC490077
- DOI: 10.1503/cmaj.1031155
Vitamin B12 (cobalamin) deficiency in elderly patients
Abstract
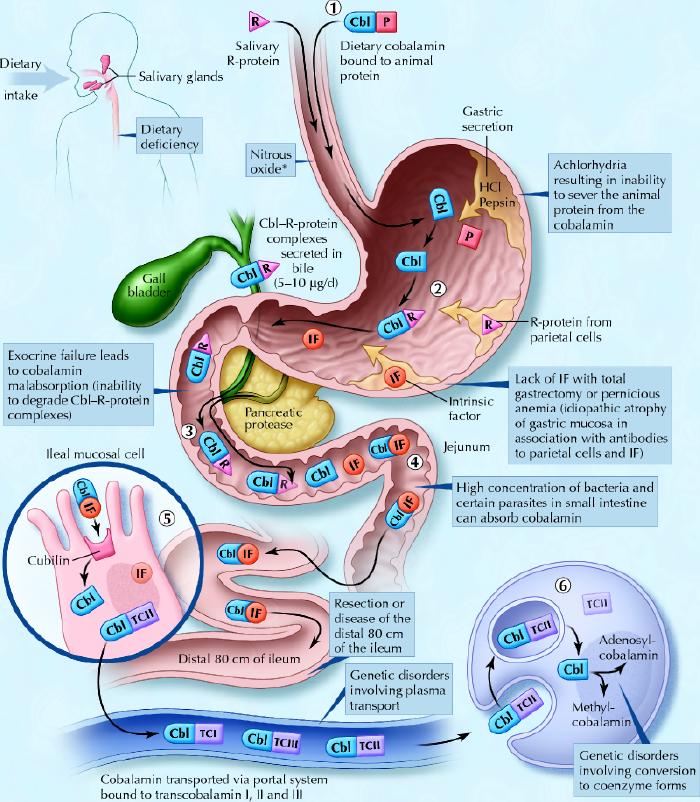
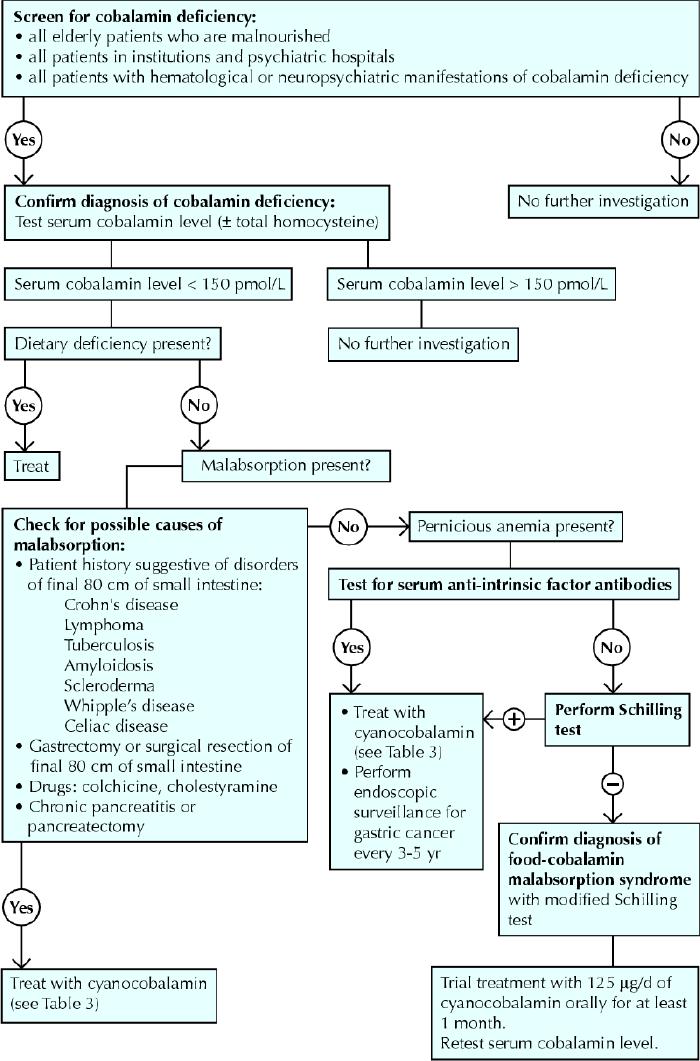
Vitamin B12 or cobalamin deficiency occurs frequently (> 20%) among elderly people, but it is often unrecognized because the clinical manifestations are subtle; they are also potentially serious, particularly from a neuropsychiatric and hematological perspective. Causes of the deficiency include, most frequently, food-cobalamin malabsorption syndrome (> 60% of all cases), pernicious anemia (15%-20% of all cases), insufficient dietary intake and malabsorption. Food-cobalamin malabsorption, which has only recently been identified as a significant cause of cobalamin deficiency among elderly people, is characterized by the inability to release cobalamin from food or a deficiency of intestinal cobalamin transport proteins or both. We review the epidemiology and causes of cobalamin deficiency in elderly people, with an emphasis on food-cobalamin malabsorption syndrome. We also review diagnostic and management strategies for cobalamin deficiency.
Figures
Comment in
-
Cobalamin deficiency in elderly patients.CMAJ. 2005 Feb 15;172(4):448-50; author reply 451. doi: 10.1503/cmaj.1041365. CMAJ. 2005. PMID: 15710919 Free PMC article. No abstract available.
-
Cobalamin deficiency in elderly patients.CMAJ. 2005 Feb 15;172(4):450-1; author reply 451. doi: 10.1503/cmaj.1041424. CMAJ. 2005. PMID: 15710922 Free PMC article. No abstract available.
-
Cobalamin deficiency in elderly patients.CMAJ. 2005 Feb 15;172(4):450; author reply 451. doi: 10.1503/cmaj.1041367. CMAJ. 2005. PMID: 15710923 Free PMC article. No abstract available.
References
-
- Matthews JH. Cobalamin and folate deficiency in the elderly. Baillères Clin Haematol 1995;54:245-53. - PubMed
-
- Stabler SP, Allen RH, Savage DG, Lindenbaum J. Clinical spectrum and diagnosis of cobalamin deficiency. Blood 1990;76:871-81. - PubMed
-
- Reynolds EH. Neurological aspects of folate and vitamin B12 metabolism. Clin Haematol 1976;5:661-96. - PubMed
-
- Carmel R. Current concepts in cobalamin deficiency. Annu Rev Med 2000;51: 357-75. - PubMed
-
- Snow C. Laboratory Diagnosis of vitamin B12 and folate deficiency. A guide for the primary care physician. Arch Intern Med 1999;159:1289-98. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical