

Prospective randomised controlled trial of an infection screening programme to reduce the rate of preterm delivery
- PMID: 15294856
- PMCID: PMC509340
- DOI: 10.1136/bmj.38169.519653.EB
Prospective randomised controlled trial of an infection screening programme to reduce the rate of preterm delivery
Abstract
Objective: To evaluate whether a screening strategy in pregnancy lowers the rate of preterm delivery in a general population of pregnant women.
Design: Multicentre, prospective, randomised controlled trial.
Setting: Non-hospital based antenatal clinics.
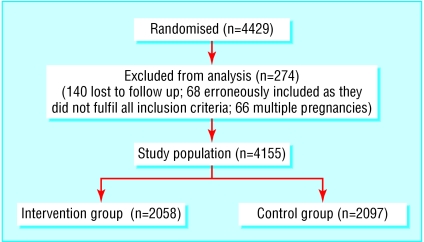
Participants: 4429 pregnant women presenting for their routine prenatal visits early in the second trimester were screened by Gram stain for asymptomatic vaginal infection. In the intervention group, the women's obstetricians received the test results and women received standard treatment and follow up for any detected infection. In the control group, the results of the vaginal smears were not revealed to the caregivers.
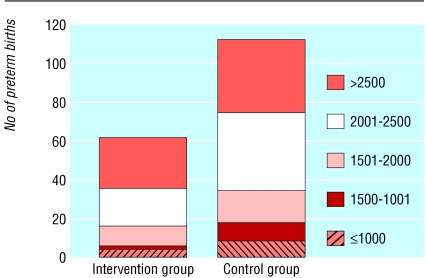
Main outcome measures: The primary outcome variable was preterm delivery at less than 37 weeks. Secondary outcome variables were preterm delivery at less than 37 weeks combined with different birth weight categories equal to or below 2500 g and the rate of late miscarriage.
Results: Outcome data were available for 2058 women in the intervention group and 2097 women in the control group. In the intervention group, the number of preterm births was significantly lower than in the control group (3.0% v 5.3%, 95% confidence interval 1.2 to 3.6; P = 0.0001). Preterm births were also significantly reduced in lower weight categories at less than 37 weeks and <or= 2500 g. Eight late miscarriages occurred in the intervention group and 15 in the control group.
Conclusion: Integrating a simple infection screening programme into routine antenatal care leads to a significant reduction in preterm births and reduces the rate of late miscarriage in a general population of pregnant women.
Figures
Comment in
-
Does screening reduce preterm births?BMJ. 2004 Aug 14;329(7462):374. doi: 10.1136/bmj.329.7462.374. BMJ. 2004. PMID: 15310607 Free PMC article. No abstract available.
References
-
- St John EB, Nelson KG, Cliver SP, Bishnio RR, Goldenberg RL. Cost of neonatal care according to gestational age at birth and survival status. Am J Obstet Gynecol 2000;182: 170-5. - PubMed
-
- Ahner R, Kohlhauser C, Bikas D, Rabl M, Langer M, Pollak A, et al. Grenzen der fetalen Lebensfähigkeit und Konsequenzen für das geburtshilfliche Management. Geburtsh Frauenheilk 2000;60: 20-5.
-
- Xu B, Rantakallio P, Jarvelin MR. Mortality and hospitalizations of 24-year-old members of the low-birthweight cohort in northern Finland. Epidemiology 1998;9: 662-5. - PubMed
-
- Petrou S, Sach T, Davidson L. The long term costs of preterm birth and low birth weight: results of a systematic review. Child Care Health Dev 2001;27: 97-115. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical