

Effectiveness of a multiple intervention to reduce antibiotic prescribing for respiratory tract symptoms in primary care: randomised controlled trial
- PMID: 15297305
- PMCID: PMC514206
- DOI: 10.1136/bmj.38182.591238.EB
Effectiveness of a multiple intervention to reduce antibiotic prescribing for respiratory tract symptoms in primary care: randomised controlled trial
Abstract
Objectives: To assess the effectiveness of a multiple intervention aimed at reducing antibiotic prescription rates for symptoms of the respiratory tract in primary care.
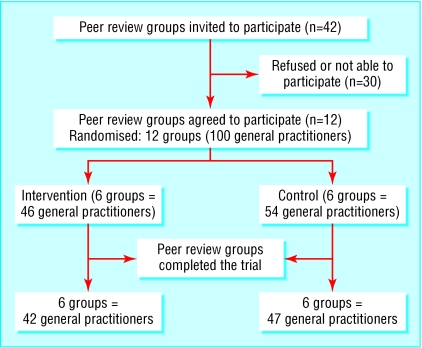
Design: Randomised controlled trial.
Subjects: Twelve peer review groups including 100 general practitioners with their collaborating pharmacists in the region of Utrecht, Netherlands.
Intervention: The intervention consisted of group education meetings, with a consensus procedure on indication for and type of antibiotics and with training in communication skills; monitoring and feedback on prescribing behaviour; group education for assistants of general practitioners and pharmacists; and education material for patients. The control group did not receive any of these elements.
Main outcome measures: Antibiotic prescription rates for acute symptoms of the respiratory tract and patients' satisfaction.
Results: 89 general practitioners completed the study (89%). At baseline, prescription rates for antibiotics for respiratory tract symptoms did not differ between intervention and control group (27% v 29%, respectively). After nine months, the prescription rates in the intervention group fell to 23%, whereas the control group's rose to 37% (mean difference in change -12%, 95% confidence interval -18.9% to -4.0%). Multilevel analysis confirmed the results of the unadjusted analysis (intervention effect -10.7%, -20.3% to -1.0%). Patients' satisfaction was high and did not differ in the two groups at baseline or after the intervention.
Conclusions: A multiple intervention reduced prescribing rates of antibiotics for respiratory tract symptoms while maintaining a high degree of satisfaction among patients. Further research should focus on the sustainability and cost effectiveness of this intervention.
Figures
References
-
- De Melker RA, Kuyvenhoven MM. Management of upper respiratory tract infections in Dutch family practice. J Fam Pract 1994;38: 353-7. - PubMed
-
- Arroll B, Kenealy T. Antibiotics for the common cold. Cochrane Database Syst Rev 2000;(2): CD000247. - PubMed
-
- Del Mar CB, Glasziou PP, Spinks AB. Antibiotics for sore throat. Cochrane Database Syst Rev 2000;(4): CD000023. - PubMed
-
- Becker L, Glazier R, McIsaac W, Smucny J. Antibiotics for acute bronchitis. Cochrane Database Syst Rev 2000;(2): CD000245. - PubMed
-
- Glasziou PP, Del Mar CB, Sanders SL, Hayem M Antibiotics for acute otitis media in children. Cochrane Database Syst Rev 2004;(1): CD000219. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical