

Racial variations in processes of care for patients with community-acquired pneumonia
- PMID: 15304197
- PMCID: PMC514714
- DOI: 10.1186/1472-6963-4-20
Racial variations in processes of care for patients with community-acquired pneumonia
Abstract
Background: Patients hospitalized with community acquired pneumonia (CAP) have a substantial risk of death, but there is evidence that adherence to certain processes of care, including antibiotic administration within 8 hours, can decrease this risk. Although national mortality data shows blacks have a substantially increased odds of death due to pneumonia as compared to whites previous studies of short-term mortality have found decreased mortality for blacks. Therefore we examined pneumonia-related processes of care and short-term mortality in a population of patients hospitalized with CAP.
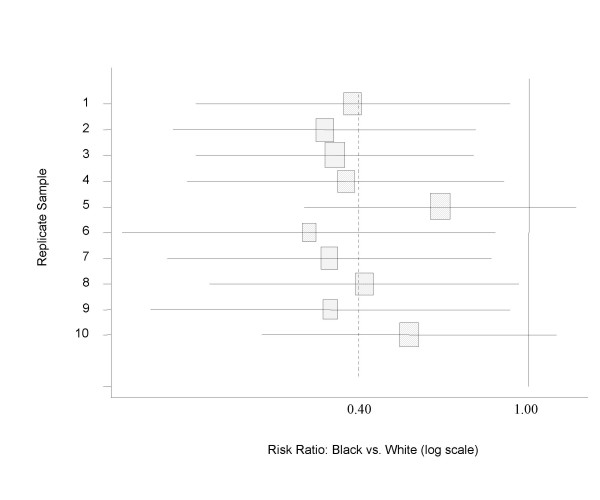
Methods: We reviewed the records of all identified Medicare beneficiaries hospitalized for pneumonia between 10/1/1998 and 9/30/1999 at one of 101 Pennsylvania hospitals, and randomly selected 60 patients at each hospital for inclusion. We reviewed the medical records to gather process measures of quality, pneumonia severity and demographics. We used Medicare administrative data to identify 30-day mortality. Because only a small proportion of the study population was black, we included all 240 black patients and randomly selected 720 white patients matched on age and gender. We performed a resampling of the white patients 10 times.
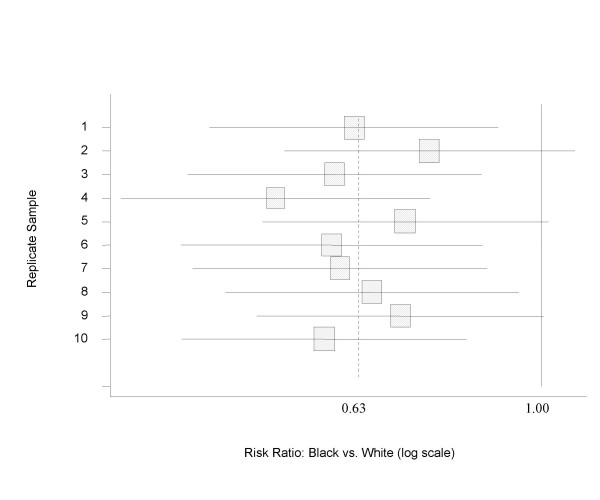
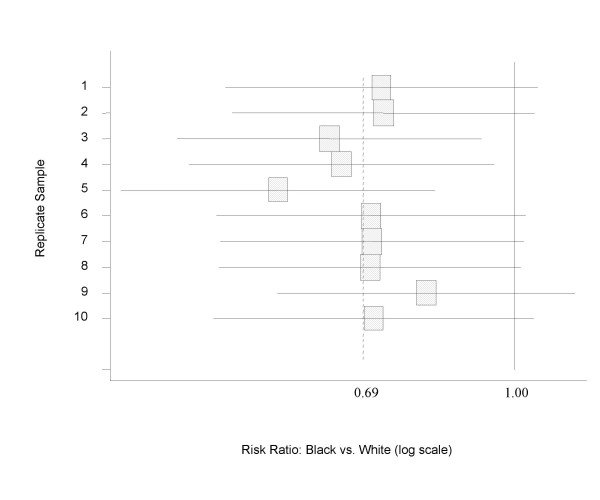
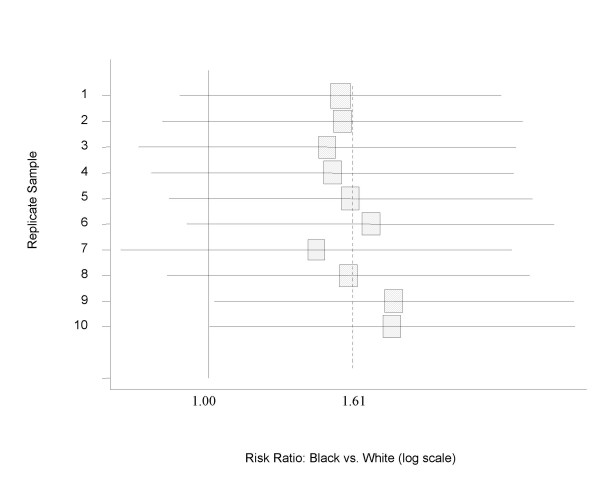
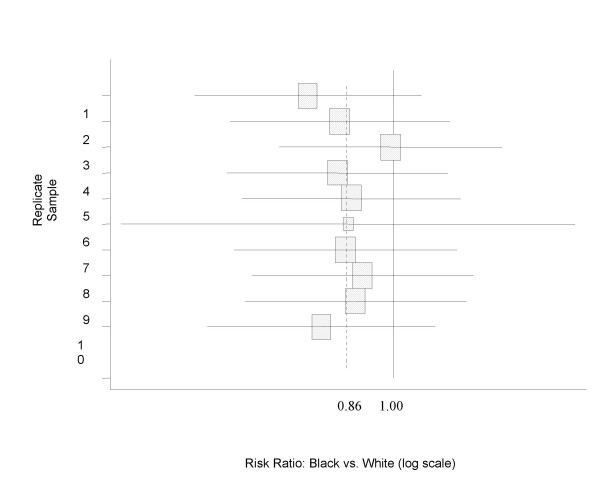
Results: Males were 43% of the cohort, and the median age was 76 years. After controlling for potential confounders, blacks were less likely to receive antibiotics within 8 hours (odds ratio with 95% confidence interval 0.6, 0.4-0.97), but were as likely as whites to have blood cultures obtained prior to receiving antibiotics (0.7, 0.3-1.5), to have oxygenation assessed within 24 hours of presentation (1.6, 0.9-3.0), and to receive guideline concordant antibiotics (OR 0.9, 0.6-1.7). Black patients had a trend towards decreased 30-day mortality (0.4, 0.2 to 1.0).
Conclusion: Although blacks were less likely to receive optimal care, our findings are consistent with other studies that suggest better risk-adjusted survival among blacks than among whites. Further study is needed to determine why this is the case.
Figures
References
-
- Anonymous Deaths: Final data for 1997. Vital Statistics Reports. 1999;47 - PubMed
-
- Group The NHLBI Working. Respiratory diseases disproportionately affecting minorities. Chest. pp. 1380–1392. - PubMed
-
- Services US Dept of Health and Human. DHHS publication 271-848-40085. 3rd. Vol. 5. Washington, DC, US Government Printing Office; 1991. Health status of minorities and low-income groups.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
