

Colonoscopic resection of lateral spreading tumours: a prospective analysis of endoscopic mucosal resection
- PMID: 15306595
- PMCID: PMC1774165
- DOI: 10.1136/gut.2003.036913
Colonoscopic resection of lateral spreading tumours: a prospective analysis of endoscopic mucosal resection
Abstract
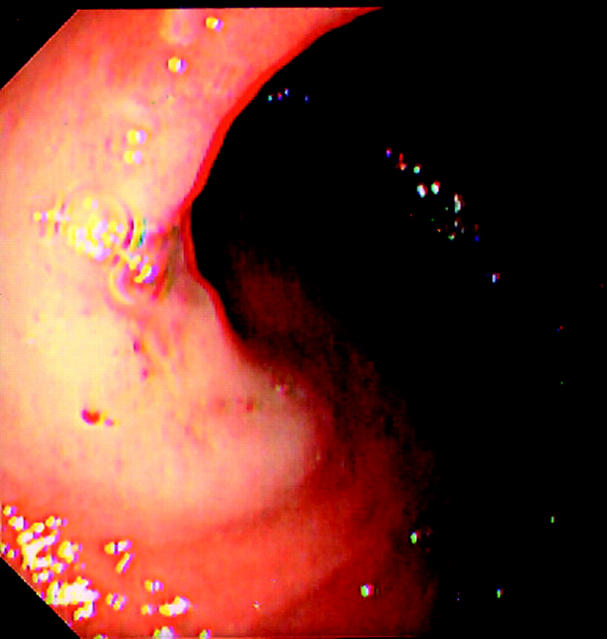
Background: Lateral spreading tumours are superficial spreading neoplasms now increasingly diagnosed using chromoscopic colonoscopy. The clinicopathological features and safety of endoscopic mucosal resection for lateral spreading tumours (G-type "aggregate" and F-type "flat") has yet to be clarified in Western cohorts.
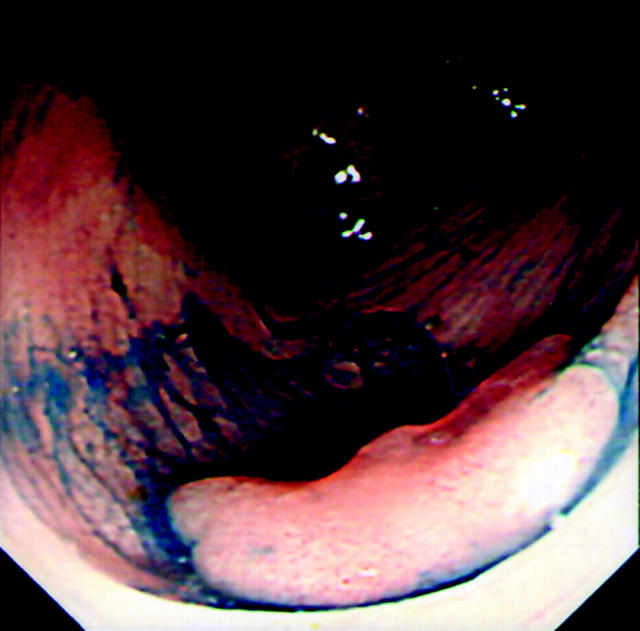
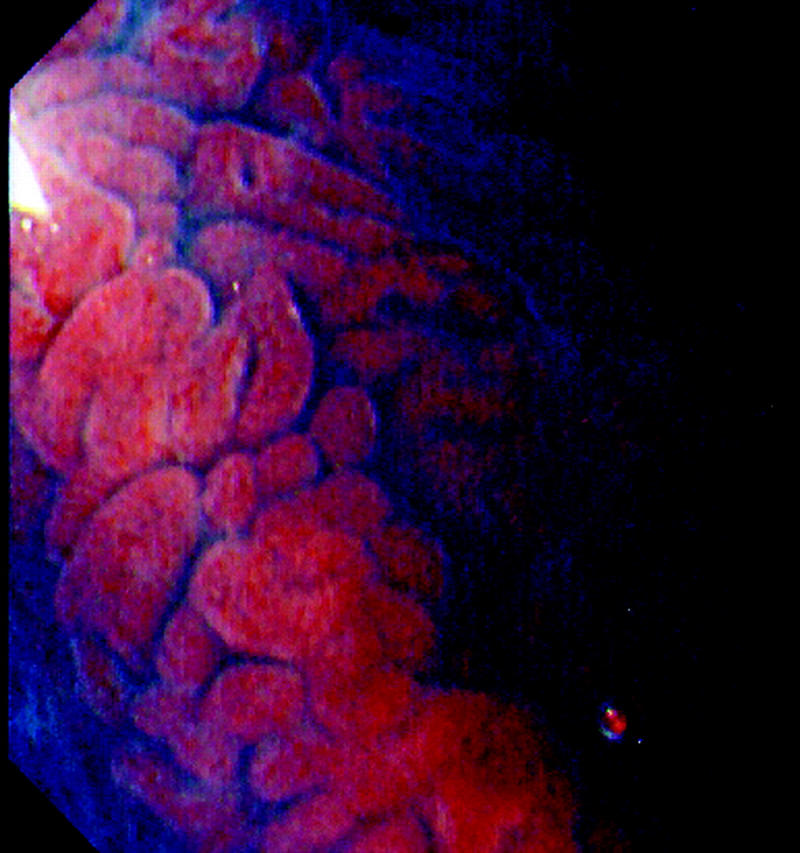
Methods: Eighty two patients underwent magnification chromoscopic colonoscopy using the Olympus CF240Z by a single endoscopist. All patients had received a previous colonoscopy where an endoscopic diagnosis of lateral spreading tumour was made. All lesions were examined initially using indigo carmine chromoscopy to delineate contour followed by crystal violet for magnification crypt pattern analysis. A 20 MHz "mini probe" ultrasound was used if T2 disease was suspected. Following endoscopic mucosal resection, patients were followed up at 3, 6, 12, and 24 months using total colonoscopy.
Results: Eighty two lateral spreading tumours were diagnosed in 80 patients (32% (26/82) F-type and 68% (56/82) G-type). G-type lesions were larger than F-type (G-type mean 42 (SD 14) mm v F-type 24 (6.4) mm; p<0.01). F-type lesions were more common in the right colon (F-type 77% (20/26) compared with G-type 39% (22/56); p<0.01) and more often associated with invasive disease (stage T2) (66% (10/15) v 33% (5/15); p<0.001). Fifty eight lesions underwent endoscopic mucosal resection (G-type 64% (37/58)/F-type 36% (21/58)). Local recurrent disease was detected in 17% of patients (10/58), all within six months of the index resection. Piecemeal resection and G-type morphology were significantly associated with recurrent disease (p<0.1). Overall "cure" rates for lateral spreading tumours using endoscopic mucosal resection at two years of follow-up was 96% (56/58).
Conclusions: Endoscopic mucosal resection for lateral spreading tumours, staged as T1, is a safe and effective treatment despite their large size. Endoscopic mucosal resection may be an alternative to surgery in selected patients.
Figures


Comment in
-
Endoscopic mucosal resection: an evolving therapeutic strategy for non-polypoid colorectal neoplasia.Gut. 2004 Sep;53(9):1222-4. doi: 10.1136/gut.2004.043281. Gut. 2004. PMID: 15306573 Free PMC article. Review. No abstract available.
-
Safety and efficacy of endoscopic mucosal resection in patients with lateral spreading tumors of the colorectum.Nat Clin Pract Gastroenterol Hepatol. 2005 Feb;2(2):78-9. doi: 10.1038/ncpgasthep0089. Nat Clin Pract Gastroenterol Hepatol. 2005. PMID: 16265123 No abstract available.
References
-
- Kudo S . Endoscopic mucosal resection of flat and depressed types of early colorectal cancer. Endoscopy 1993;25:455–61. - PubMed
-
- Hurlstone D , Korulla C, Lobo A. Colorectal laterally spreading tumors: Clinical evaluation and endoscopic strategies updated. J Gastroenterol Hepatol 2002;17:1344–5. - PubMed
-
- Okamoto T , Tanaka S, Haruma K, et al. Clinicopathological evaluation on colorectal laterally spreading tumor (LST) (in Japanese with English abstract). Nippon Geka Gakkai Zasshi 1996;93:83–9. - PubMed
-
- Hurlstone DP, Fujii T, Lobo AJ. Early detection of colorectal cancer using high-magnification chromoscopic colonoscopy. Br J Surg 2002;89:272–82. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical