

Congenital duodenal diaphragm in eight children
- PMID: 15307458
- PMCID: PMC6147924
- DOI: 10.5144/0256-4947.2004.193
Congenital duodenal diaphragm in eight children
Erratum in
- Ann Saudi Med. 2004 Nov-Dec;24(6):490
Abstract
Background: Congenital duodenal obstruction (CDO) is a common and usually easy to diagnose cause of intestinal obstruction in the newborn, except when the cause of the obstruction is a duodenal diaphragm. We describe our experience with eight children who had intrinsic duodenal obstruction secondary to a duodenal diaphragm.
Methods: The medical records of 22 children with the diagnosis of congenital intrinsic duodenal obstruction were reviewed for age at diagnosis, sex, gestation, birth weight, clinical features, associated anomalies, method of diagnosis, treatment and outcome. Operative findings and procedures were obtained from the operative notes.
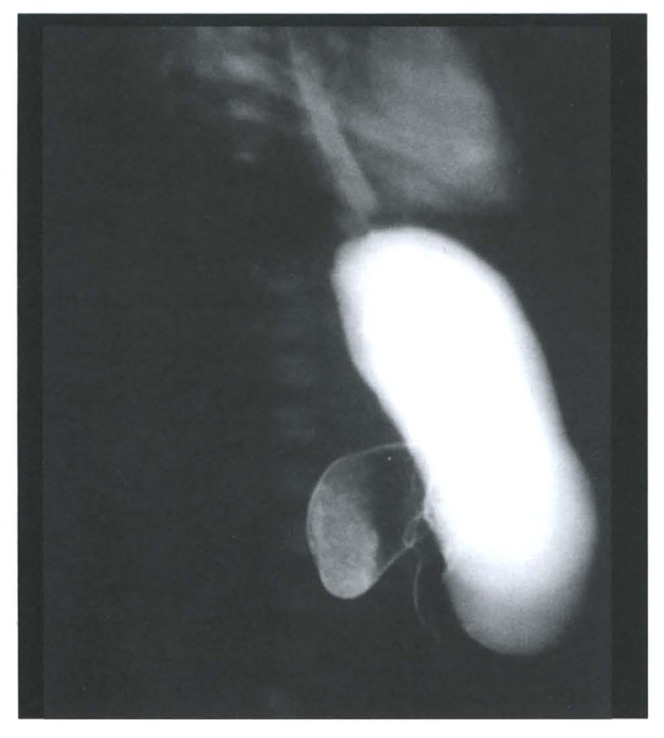
Results: Eight of the 22 children (36.4%) had congenital duodenal diaphragm (CDD). In all children, the diagnosis was made from plain abdominal X-ray, which showed the classic double-bubble appearance, and barium meal, which showed duodenal obstruction. Four patients had associated anomalies, including two with Down's syndrome. Intraoperatively, five patients were found to have duodenal diaphragm with a central hole, while the other three had complete duodenal diaphragms. Postoperatively, all patients did well. Six required total parenteral nutrition.
Conclusions: The 100% survival rate among these children is comparable to that in Western countries, and can be attributed to the lack of major associated abnormalities, good perioperative management, and the availability of total parenteral nutrition.
Figures



Similar articles
-
[Congenital duodenal obstruction - part II].Med Wieku Rozwoj. 2004 Jul-Sep;8(3 Pt 2):751-9. Med Wieku Rozwoj. 2004. PMID: 15858247 Polish.
-
Congenital duodenal obstruction in children: a decade's experience.Eur J Pediatr Surg. 2008 Apr;18(2):93-7. doi: 10.1055/s-2008-1038478. Eur J Pediatr Surg. 2008. PMID: 18437652
-
[Experiences with congenital duodenal obstruction in the Sophia Kinderziekenhuis].Ned Tijdschr Geneeskd. 1991 Jul 13;135(28):1272-5. Ned Tijdschr Geneeskd. 1991. PMID: 1830640 Dutch.
-
[Congenital duodenal obstruction -- Part I].Med Wieku Rozwoj. 2004 Jul-Sep;8(3 Pt 2):745-50. Med Wieku Rozwoj. 2004. PMID: 15858246 Review. Polish.
-
Congenital duodenal membrane: a ten-year review.Acta Paediatr Taiwan. 1999 Mar-Apr;40(2):70-4. Acta Paediatr Taiwan. 1999. PMID: 10910590 Review.
Cited by
-
Congenital duodenal diaphragm and enteroliths: A Unique complication.J Indian Assoc Pediatr Surg. 2009 Oct;14(4):226-7. doi: 10.4103/0971-9261.59609. J Indian Assoc Pediatr Surg. 2009. PMID: 20419028 Free PMC article.
-
Congenital duodenal obstruction with delayed presentation: seven years of experience.Arch Med Sci. 2016 Oct 1;12(5):1023-1027. doi: 10.5114/aoms.2016.60045. Epub 2016 May 19. Arch Med Sci. 2016. PMID: 27695493 Free PMC article.
-
Delayed presentation of duodenal atresia.Afr J Paediatr Surg. 2023 Apr-Jun;20(2):97-101. doi: 10.4103/ajps.ajps_66_21. Afr J Paediatr Surg. 2023. PMID: 36960502 Free PMC article.
-
Case report of a congenital duodenal transverse septum causing partial obstruction.Medicine (Baltimore). 2017 Oct;96(42):e7093. doi: 10.1097/MD.0000000000007093. Medicine (Baltimore). 2017. PMID: 29049170 Free PMC article.
-
Tips and Tricks in the Laparoscopic Treatment of Type I Duodenal Atresia: Description of a Technique.Children (Basel). 2025 Apr 17;12(4):517. doi: 10.3390/children12040517. Children (Basel). 2025. PMID: 40310202 Free PMC article.
References
-
- Huang FC, Chuang JH, Shich CS. Congenital duodenal membrane: a ten–year review. Acta paediatr Taiwan. 1999;40:70–74. - PubMed
-
- Lehur PA, Poisson J, Lamontagne L, Haddad H. Congenital diaphragm of the duodenum in an adult: a case report. Can J Surg. 1983;26:559–560. - PubMed
-
- Rowe MI, Buckner D, Clatworthy HW. Windsock web of the duodenum. Am J Surg. 1968;116:444–149. - PubMed
-
- Horgan PG, Horgan AF, O’Donnell JA. The neonatal windsock web-a case report and description of a new technique for its operative excision. Irish J Med Sci. 1990;159:110. - PubMed
-
- Al-Salem AH, Khawaja S, Grant C, Dawodu A. Congenital duodenal obstruction: Problems in the diagnosis and management. J Pediatr Surg. 1989;24:1247–1249. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources