

Performance of six severity-of-illness scores in cancer patients requiring admission to the intensive care unit: a prospective observational study
- PMID: 15312218
- PMCID: PMC522839
- DOI: 10.1186/cc2870
Performance of six severity-of-illness scores in cancer patients requiring admission to the intensive care unit: a prospective observational study
Abstract
Introduction: The aim of this study was to evaluate the performance of five general severity-of-illness scores (Acute Physiology and Chronic Health Evaluation II and III-J, the Simplified Acute Physiology Score II, and the Mortality Probability Models at admission and at 24 hours of intensive care unit [ICU] stay), and to validate a specific score - the ICU Cancer Mortality Model (CMM) - in cancer patients requiring admission to the ICU.
Methods: A prospective observational cohort study was performed in an oncological medical/surgical ICU in a Brazilian cancer centre. Data were collected over the first 24 hours of ICU stay. Discrimination was assessed by area under the receiver operating characteristic curves and calibration was done using Hosmer-Lemeshow goodness-of-fit H-tests.
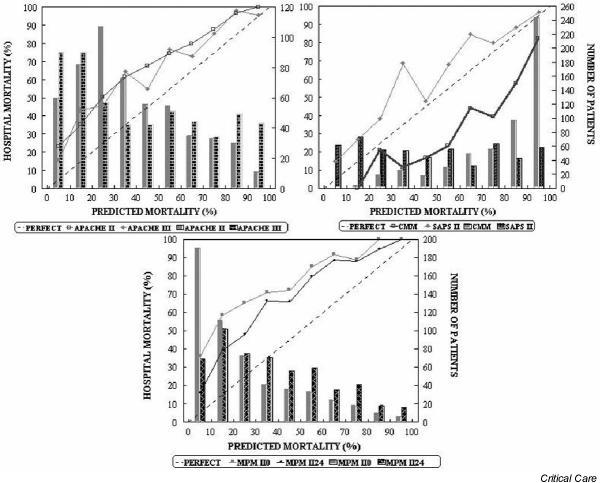
Results: A total of 1257 consecutive patients were included over a 39-month period, and 715 (56.9%) were scheduled surgical patients. The observed hospital mortality was 28.6%. Two performance analyses were carried out: in the first analysis all patients were studied; and in the second, scheduled surgical patients were excluded in order to better compare CMM and general prognostic scores. The results of the two analyses were similar. Discrimination was good for all of the six studied models and best for Simplified Acute Physiology Score II and Acute Physiology and Chronic Health Evaluation III-J. However, calibration was uniformly insufficient (P < 0.001). General scores significantly underestimated mortality (in comparison with the observed mortality); this was in contrast to the CMM, which tended to overestimate mortality.
Conclusion: None of the model scores accurately predicted outcome in the present group of critically ill cancer patients. In addition, there was no advantage of CMM over the other general models.
Figures

References
-
- Sculier J-P. Intensive care and oncology. Support Care Cancer. 1995;3:93–105. - PubMed
-
- Azoulay E, Pochard F, Chevret S, Vinsonneau C, Garrouste M, Cohen Y, Thuong M, Paugam C, Apperre C, De Cagny B, Brun F, Bornstain C, Parrot A, Thamion F, Lacherade JC, Bouffard Y, Le Gall J-R, Herve C, Grassin M, Zittoun R, Schlemmer B, Dhainaut JF, for the PROTOCETIC Group Compliance with triage to intensive care recommendations. Crit Care Med. 2001;29:2132–2136. doi: 10.1097/00003246-200111000-00014. - DOI - PubMed
-
- Benoit DD, Wandewoude KH, Decruyenaere JM, Hoste EA, Colardyn FA. Outcome and early prognostic indicators in patients with a hematologic malignancy admitted to the intensive care unit for a life-threatening complication. Crit Care Med. 2003;31:104–112. doi: 10.1097/00003246-200301000-00017. - DOI - PubMed
-
- Staudinger T, Stoiser B, Mullner M, Locker GJ, Laczika K, Knapp S, Burgmann H, Wilfing A, Kofler J, Thalhammer F, Frass M. Outcome and prognostic factors in critically ill cancer patients admitted to the intensive care unit. Crit Care Med. 2000;28:1322–1328. doi: 10.1097/00003246-200005000-00011. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
