

Procalcitonin and C-reactive protein during systemic inflammatory response syndrome, sepsis and organ dysfunction
- PMID: 15312223
- PMCID: PMC522844
- DOI: 10.1186/cc2877
Procalcitonin and C-reactive protein during systemic inflammatory response syndrome, sepsis and organ dysfunction
Abstract
Introduction: Both C-reactive protein (CRP) and procalcitonin (PCT) are accepted sepsis markers. However, there is still some debate concerning the correlation between their serum concentrations and sepsis severity. We hypothesised that PCT and CRP concentrations are different in patients with infection or with no infection at a similar severity of organ dysfunction or of systemic inflammatory response.
Patients and methods: One hundred and fifty adult intensive care unit patients were observed consecutively over a period of 10 days. PCT, CRP and infection parameters were compared among the following groups: no systemic inflammatory response syndrome (SIRS) (n = 15), SIRS (n = 15), sepsis/SS (n = 71) (including sepsis, severe sepsis and septic shock [n = 34, n = 22 and n = 15]), and trauma patients (n = 49, no infection).
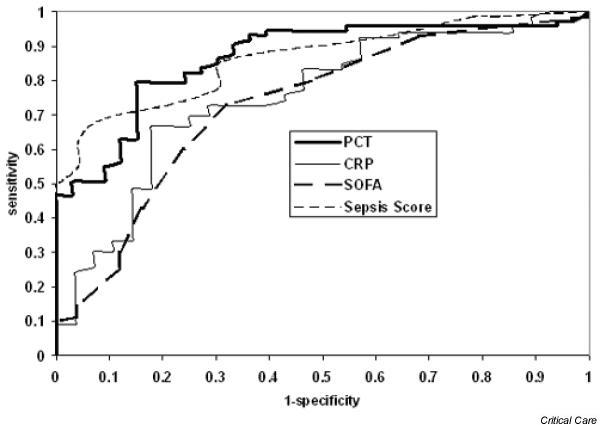
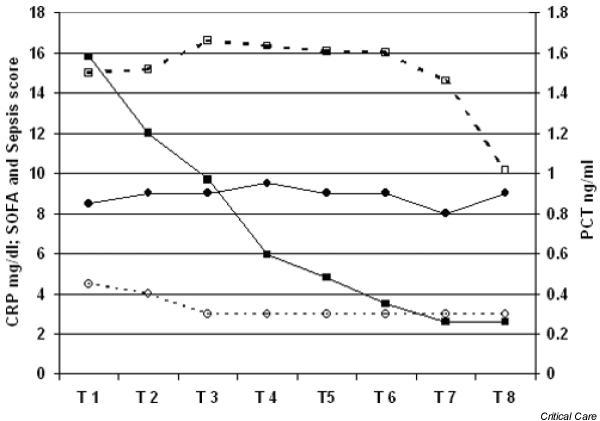
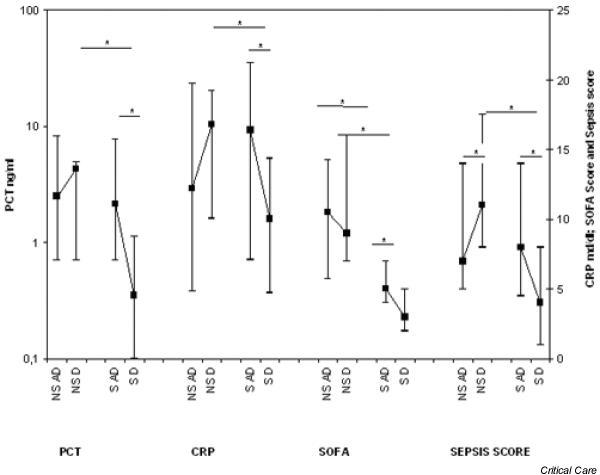
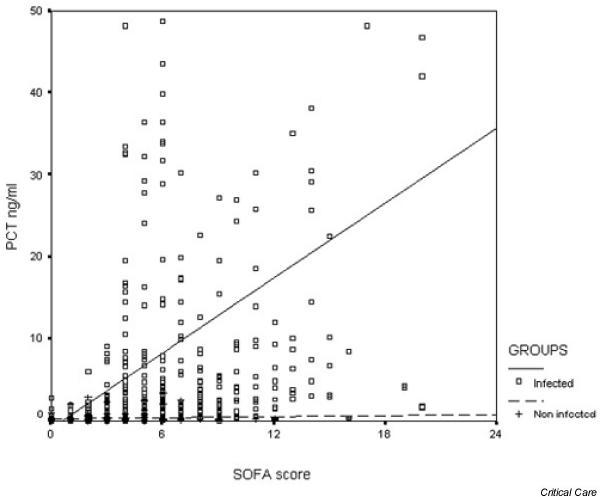
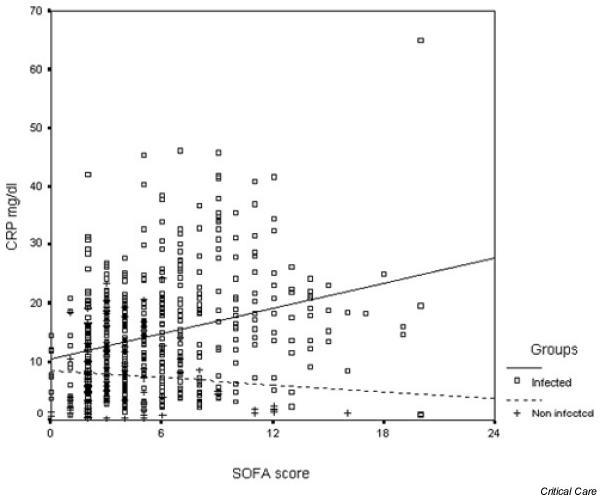
Results: PCT and CRP concentrations were higher in patients in whom infection was diagnosed at comparable levels of organ dysfunction (infected patients, regression of median [ng/ml] PCT = -0.848 + 1.526 sequential organ failure assessment [SOFA] score, median [mg/l] CRP = 105.58 + 0.72 SOFA score; non-infected patients, PCT = 0.27 + 0.02 SOFA score, P < 0.0001; CRP = 84.53 - 0.19 SOFA score, P < 0.005), although correlation with the SOFA score was weak (R = 0.254, P < 0.001 for PCT, and R = 0.292, P < 0.001 for CRP). CRP levels were near their maximum already during lower SOFA scores, whereas maximum PCT concentrations were found at higher score levels (SOFA score > 12).PCT and CRP concentrations were 1.58 ng/ml and 150 mg/l in patients with sepsis, 0.38 ng/ml and 51 mg/l in the SIRS patients (P < 0.05, Mann-Whitney U-test), and 0.14 ng/ml and 72 mg/l in the patients with no SIRS (P < 0.05). The kinetics of both parameters were also different, and PCT concentrations reacted more quickly than CRP.
Conclusions: PCT and CRP levels are related to the severity of organ dysfunction, but concentrations are still higher during infection. Different sensitivities and kinetics indicate a different clinical use for both parameters.
Figures

References
-
- Yentis SM, Soni N, Sheldon J. C-reactive protein as an indicator of resolution of sepsis in the intensive care unit. Intensive Care Med. 1995;21:602–605. - PubMed
-
- Matson A, Soni N, Sheldon J. C-reactive protein as a diagnostic test of sepsis in the critically ill. Anaesth Intensive Care. 1991;19:182–186. - PubMed
-
- Al-Nawas B, Krammer I, Shah PM. Procalcitonin in diagnosis of severe infections. Eur J Med Res. 1996;1:331–333. - PubMed
-
- Gramm HJ, Beier W, Zimmermann J, Oedra N, Hannemann L, Boese-Landgraf J. Procalcitonin (ProCT) – a biological marker of the inflammatory response with prognostic properties. Clin Intensive Care. 1995;[Abstract] 6(Suppl 2):71.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
