

Tracheostomy timing and the duration of weaning in patients with acute respiratory failure
- PMID: 15312227
- PMCID: PMC522847
- DOI: 10.1186/cc2885
Tracheostomy timing and the duration of weaning in patients with acute respiratory failure
Abstract
Introduction: The effect of various airway management strategies, such as the timing of tracheostomy, on liberation from mechanical ventilation (MV) is uncertain. We tested the hypothesis that tracheostomy, when performed prior to active weaning, does not influence the duration of weaning or of MV in comparison with a more selective use of tracheostomy.
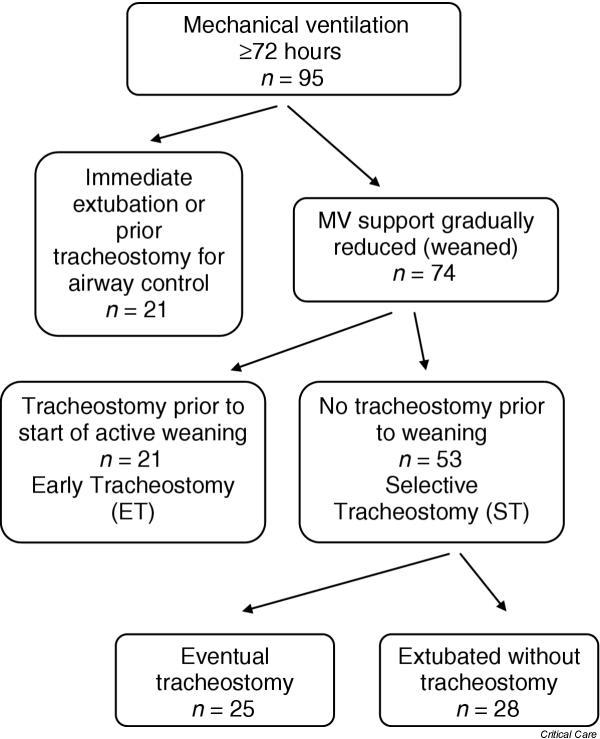
Patients and methods: In this observational prospective cohort study, surgical patients requiring >or= 72 hours of MV were followed prospectively. Patients undergoing tracheostomy prior to any active weaning attempts (early tracheostomy [ET]) were compared with patients in whom initial weaning attempts were made with the endotracheal tube in place (selective tracheostomy [ST]).
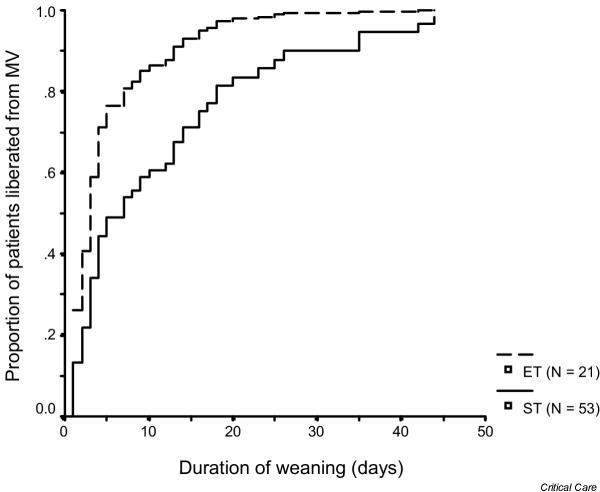
Results: We compared the duration of weaning, the total duration of MV and the frequency of fatigue and pneumonia. Seventy-four patients met inclusion criteria. Twenty-one patients in the ET group were compared with 53 patients in the ST group (47% of whom ultimately underwent tracheostomy). The median duration of weaning was shorter (3 days versus 6 days, P = 0.05) in patients in the ET group than in the ST group, but the duration of MV was not (median [interquartile range], 11 days [9-26 days] in the ET group versus 13 days [8-21 days] in the ST group). The frequencies of fatigue and pneumonia were lower in the ET group patients.
Discussion: Determining the ideal timing of tracheostomy in critically ill patients has been difficult and often subjective. To standardize this process, it is important to identify objective criteria to identify patients most likely to benefit from the procedure. Our data suggest that in surgical patients with resolving respiratory failure, a patient who meets typical criteria for a trial of spontaneous breathing but is not successfully extubated within 24 hours may benefit from a tracheostomy. Our data provide a framework for the conduct of a clinical trial in which tracheostomy timing can be assessed for its impact on the duration of weaning.
Conclusion: Tracheostomy prior to active weaning may hasten liberation from ventilation and reduce complications. However, this does not reduce the overall duration of MV.
Figures
References
-
- Whited RE. A prospective study of laryngotracheal sequelae in long-term intubation. Laryngoscope. 1984;94:367–377. - PubMed
-
- Torres A, Gatell JM, Aznar E, el Ebiary M, Puig dlB, Gonzalez J, Ferrer M, Rodriguez-Roisin R. Re-intubation increases the risk of nosocomial pneumonia in patients needing mechanical ventilation. Am J Respir Crit Care Med. 1995;152:137–141. - PubMed
-
- Rodriguez JL, Steinberg SM, Luchetti FA, Gibbons KJ, Taheri PA, Flint LM. Early tracheostomy for primary airway management in the surgical critical care setting. Surgery. 1990;108:655–659. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
