

doi: 10.1186/1468-6708-5-7.
Individualizing therapy - in search of approaches to maximize the benefit of drug treatment (II)
Affiliations
- PMID: 15312237
- PMCID: PMC514911
- DOI: 10.1186/1468-6708-5-7
Item in Clipboard
Individualizing therapy - in search of approaches to maximize the benefit of drug treatment (II)
Curr Control Trials Cardiovasc Med.
.
Abstract
Adjusting drug therapy to the individual, a common approach in clinical practice, has evolved from 1) dose adjustments based on clinical effects to 2) dose adjustments made in response to drug levels and, more recently, to 3) dose adjustments based on deoxyribonucleic acid (DNA) sequencing of drug-metabolizing enzyme genes, suggesting a slow drug metabolism phenotype. This development dates back to the middle of the 20(th )century, when several different drugs were administered on the basis of individual plasma concentration measurements. Genetic control of drug metabolism was well established by the 1960s, and pharmakokinetic-based individualized therapy was in use by 1973.
Figures
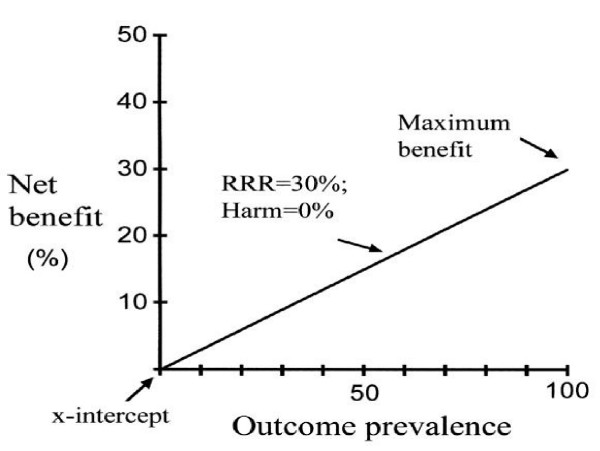
Basic relationships. Net benefit is plotted as a function of outcome prevalence. The line represents the relationship with the assumption of a relative risk reduction of 30% and treatment harm of 0%. The line is the maximum net benefit that can be attained at any given outcome prevalence. The x-intercept, or benefit threshold, represents the outcome prevalence at which net benefit will accrue to individuals and the population as a whole. The point of maximum benefit occurs when the outcome prevalence is 100%; at this point, if harm is absent, the net benefit or efficiency of treatment equals the relative risk reduction or efficacy of that treatment. Benefit decreases proportionately as a function of outcome prevalence.
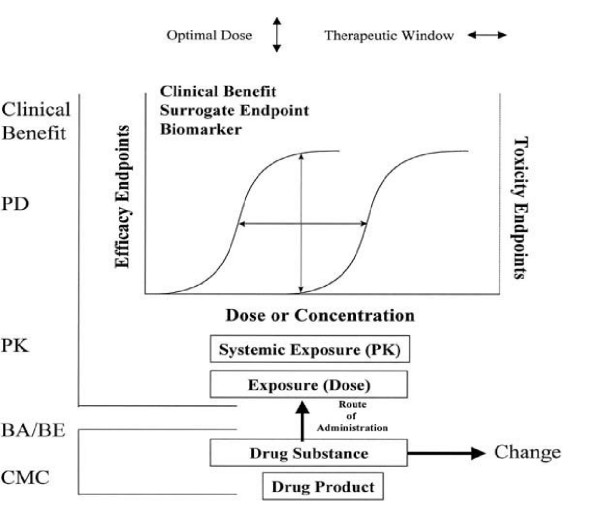
Exposure-response relationships. Relationships between (1) drug substance and drug product, (2) exposure expressed as dose or systemic exposure on log scale, and (3) positive (efficacy) or negative (toxicity) outcomes. These outcomes may be measured by clinical end points, surrogate endpoints, or biomarkers. The relationships between exposure and outcomes define the optimal dose and therapeutic window. The term change introduces the concept of equivalence in outcomes before or after a specified change (eg, generic substitution, postapproval manufacturing change). CMC, Chemistry, manufacturing, and controls; BA/BE, bioavailability and bioequivalence; PK, pharmacokinetics; PD, pharmacodynamics.
Similar articles
-
How to manage individualized drug therapy: application of pharmacogenetic knowledge of drug metabolism and transport.Clin Chem Lab Med. 2000 Sep;38(9):869-76. doi: 10.1515/CCLM.2000.126. Clin Chem Lab Med. 2000. PMID: 11097342 Review.
-
[State of the art of pharmacogenetic diagnostics in drug therapy].Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2006 Oct;49(10):995-1003. doi: 10.1007/s00103-006-0045-1. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2006. PMID: 17013776 Review. German.
-
Clinical implications of pharmacogenetics of cytochrome P450 drug metabolizing enzymes.Biochim Biophys Acta. 2007 Mar;1770(3):489-94. doi: 10.1016/j.bbagen.2006.09.019. Epub 2006 Oct 4. Biochim Biophys Acta. 2007. PMID: 17113714 Review.
-
Anticancer Drug Development: The Way Forward.Oncologist. 1996;1(3):180-181. Oncologist. 1996. PMID: 10387985
-
[Pharmacogenomics: the quest for individualized therapy].Rev Neurol. 2004 Dec 1-15;39(11):1063-71. Rev Neurol. 2004. PMID: 15597270 Review. Spanish.
Cited by
-
Methodological considerations in the design of trials for safety assessment of new drugs and chemical entities.Curr Control Trials Cardiovasc Med. 2005 Feb 3;6(1):1. doi: 10.1186/1468-6708-6-1. Curr Control Trials Cardiovasc Med. 2005. PMID: 15691384 Free PMC article. No abstract available.
-
Precision Dosing Priority Criteria: Drug, Disease, and Patient Population Variables.Front Pharmacol. 2020 Apr 22;11:420. doi: 10.3389/fphar.2020.00420. eCollection 2020. Front Pharmacol. 2020. PMID: 32390828 Free PMC article. Review.
References
-
- Wuth O. Rational bromide treatment: new methods for its control. JAMA. 1927;88:2031–2017.
-
- Shannon JA. The study of antimalarials and antimalarial activity in human malarias. Harvey Lectures Series. 1946;41:43–8. - PubMed
-
- Buchthal F, Svensmark O, Schiller PJ. Clinical and electroencephalographic correlation with serum levels of diphenylhydantoin. Arch Neurol. 1960;2:624–63. - PubMed
-
- Kalow W. Pharmacogenetics: heredity and response to drugs. Philadelphia: Saunders. 1962.
LinkOut - more resources
Full Text Sources
