

Thrombus formation during intracranial aneurysm coil placement: treatment with intra-arterial abciximab
- PMID: 15313699
- PMCID: PMC7976541
Thrombus formation during intracranial aneurysm coil placement: treatment with intra-arterial abciximab
Abstract
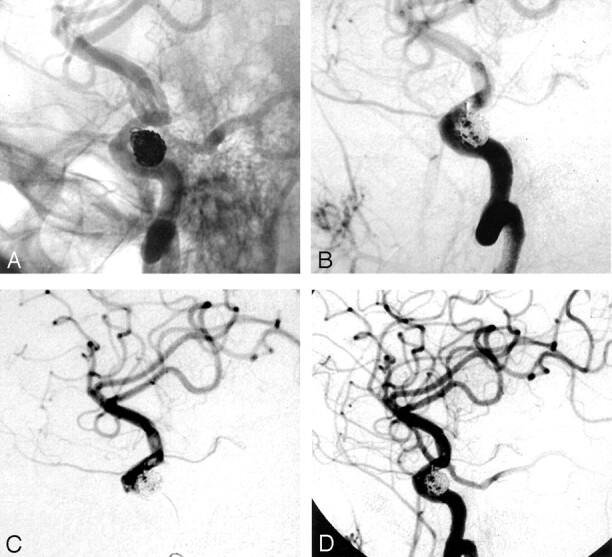
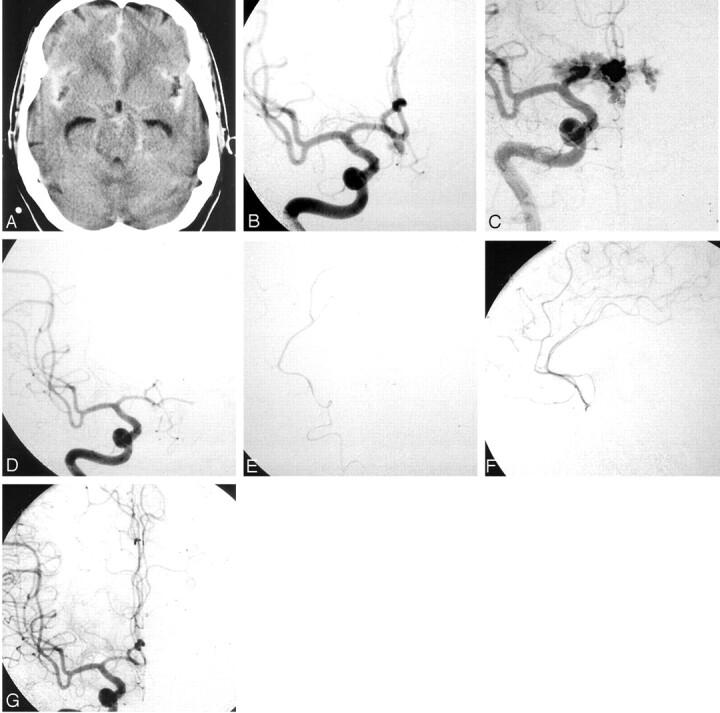
Background and purpose: The management of thrombus formation during coil placement in an intracranial aneurysm is important in minimizing periprocedural morbidity and mortality. We report on seven cases in which the primary treatment for thrombus formation during such coil placement was intra-arterial abciximab infusion.
Methods: Clinical and radiologic records of 100 consecutive patients who underwent coil placement in intracranial aneurysms at our institution during a 1-year period were reviewed. We identified seven cases (four ruptured aneurysms, three unruptured aneurysms) in which thrombus formation occurred during the procedure.
Results: Intra-arterial abciximab infusion, up to 5 mg, completely dissolved the thrombus in four of seven patients and almost completely dissolved it in two. In one patient with distal emboli, recanalization was not achieved. In two patients, an intravenous bolus of abciximab without 12-hour infusion was also given adjunctively. In one patient, leakage of contrast material occurred; this was related to the intra-arterial infusion. Clinically, no new neurologic deficits were directly related to the intra-arterial abciximab infusion. Six patients had good clinical outcome, and one patient died.
Conclusion: Relatively low-dose, intra-arterial abciximab infusion can immediately dissolve an acute thrombus that forms during intracranial aneurysm coil placement. Although neither the optimal dose of intra-arterial abciximab nor the need to supplement the intra-arterial infusion with intravenous administration was established, we preliminarily found that low-dose intra-arterial abciximab infusion may be relatively effective and safe in this setting, even in patients with acute subarachnoid hemorrhage.
Figures
References
-
- F Vinuela, Duckwiler G, Mawad M. Guglielmi detachable coil embolization of acute intracranial aneurysm: perioperative anatomical and clinical outcome in 403 patients. J Neurosurg 1997;86:475–482 - PubMed
-
- Eskridge JM, Song JK. Endovascular embolization of 150 basilar tip aneurysms with Guglielmi detachable coils: results of the Food and Drug Administration multicenter clinical trial. J Neurosurg 1998;89:81–86 - PubMed
-
- Cognard C, Weill A, Castaings L, et al. Intracranial berry aneurysms: angiographic and clinical results after endovascular treatment. Radiology 1998;206:499–510 - PubMed
-
- Debrun GM, Aletich VA, Kehrli P, et al., Selection of cerebral aneurysms for treatment using Guglielmi detachable coils: the preliminary University of Illinois at Chicago experience. Neurosurgery 1998;43:1281–1295; discussion 1296–1297 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical