

Viral infections in relation to age, atopy, and season of admission among children hospitalized for wheezing
- PMID: 15316497
- PMCID: PMC7185400
- DOI: 10.1016/j.jaci.2004.04.006
Viral infections in relation to age, atopy, and season of admission among children hospitalized for wheezing
Abstract
Background: Viral respiratory tract infections and atopy are associated with attacks of wheezing during childhood. However, information about the relationship between viral infections and atopy among children whose attacks of wheezing lead to hospitalization is unclear.
Objective: To evaluate the prevalence of viral respiratory tract pathogens among infants and children hospitalized for wheezing and to analyze the results in relation to the patient's age, atopic characteristics, and season of admission.
Methods: This was a case-control study of children (age 2 months to 18 years) admitted for wheezing to the University of Virginia Medical Center over a period of 12 months. Children without wheezing were enrolled as controls. Nasal secretions were evaluated for viral pathogens by using cultures, PCR tests, and antigen detection. Total IgE and specific IgE antibody to common aeroallergens was measured in serum.
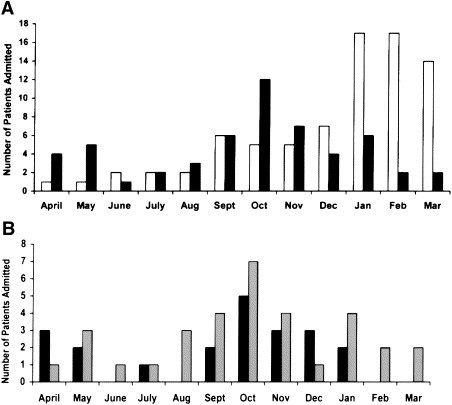
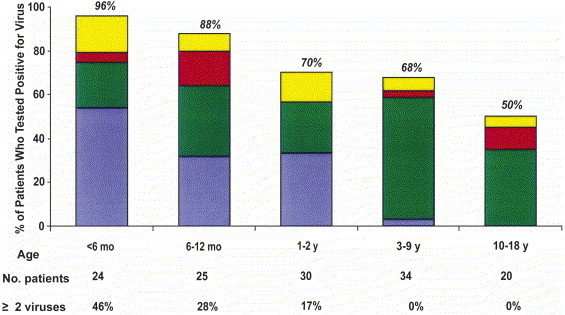
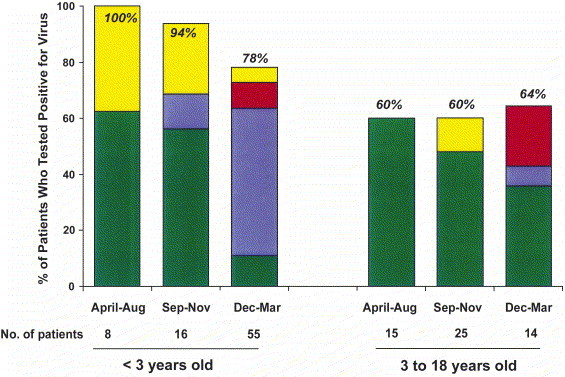
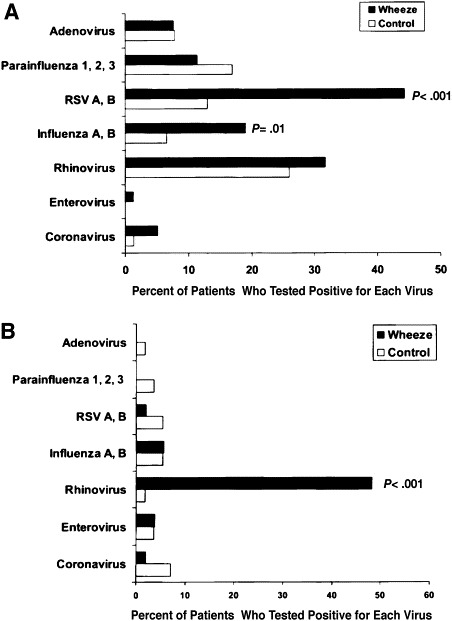
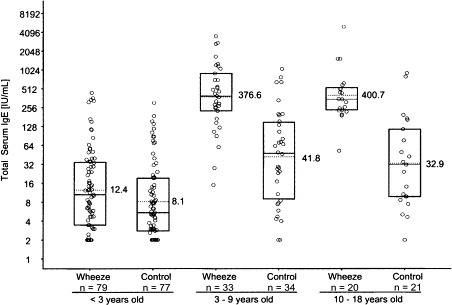
Results: Seventy percent of children hospitalized for wheezing before age 3 years (n=79) were admitted between December and March, whereas 46% of children age 3 to 18 years (n=54) were hospitalized between September and November. Among children younger than 3 years, viral pathogens were detected in 84% (66/79) of wheezing children and 55% (42/77) of controls (P <.001). Respiratory syncytial virus was the dominant pathogen during the winter months, but rhinovirus was more common during other months. Total serum IgE levels were generally low, and values from wheezing and control subjects overlapped considerably. Among children 3 years and older, 61% (33/54) of subjects admitted for wheezing tested positive for virus (predominantly rhinovirus), compared with 21% (12/56) of controls (P <.001). The total serum IgE values among wheezing children (geometric mean, 386 IU/mL; 95% CI, 259-573) were substantially elevated compared with those of controls (geometric mean, 38 IU/mL; 95% CI, 26-56; P <.001). A significantly higher percentage of wheezing children compared with controls was sensitized to at least 1 of the inhaled allergens tested: 84% (36/43) compared with 33% (15/45; P <.001). The atopic characteristics of wheezing children who tested positive or negative for virus were similar.
Conclusions: Viral infections were the dominant risk factor for wheezing among children hospitalized before 3 years of age. By comparison, a large majority of the wheezing children age 3 to 18 years had striking atopic characteristics that may be critical as a risk factor for hospitalization and an adverse response to viral infections, especially infections caused by rhinovirus.
Figures
Comment in
-
The spectrum of severe wheezing in childhood.J Allergy Clin Immunol. 2004 Aug;114(2):236-8. doi: 10.1016/j.jaci.2004.05.059. J Allergy Clin Immunol. 2004. PMID: 15316496 Free PMC article. No abstract available.
-
Origins of atopy in pediatric asthma.J Allergy Clin Immunol. 2005 Feb;115(2):425-6; author reply 426. doi: 10.1016/j.jaci.2004.10.037. J Allergy Clin Immunol. 2005. PMID: 15696110 No abstract available.
-
Human metapneumovirus infection in children hospitalized for wheezing.J Allergy Clin Immunol. 2005 Jun;115(6):1311-2. doi: 10.1016/j.jaci.2005.02.001. J Allergy Clin Immunol. 2005. PMID: 15940152 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention Measuring childhood asthma prevalence before and after the 1997 redesign of the National Health Interview Survey—United States. MMWR Morb Mortal Wkly Rep. 2000;49:908–911. - PubMed
-
- Loyano P., Sullivan S.D., Smith D.H., Weiss K.B. The economic burden of asthma in US children: estimates from the National Medical Expenditure Survey. J Allergy Clin Immunol. 1999;104:957–963. - PubMed
-
- Gergen P.J. Understanding the economic burden of asthma. J Allergy Clin Immunol. 2001;107:445–485. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
