

Chimerism and tolerance in transplantation
- PMID: 15319473
- PMCID: PMC521985
- DOI: 10.1073/pnas.0404829101
Chimerism and tolerance in transplantation
Abstract
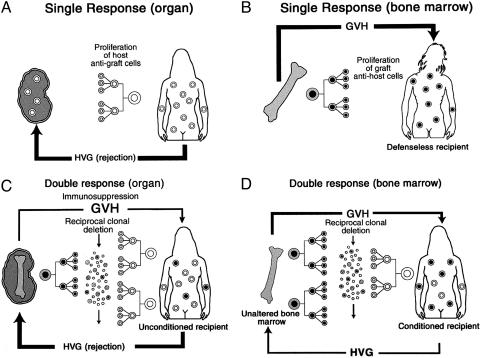
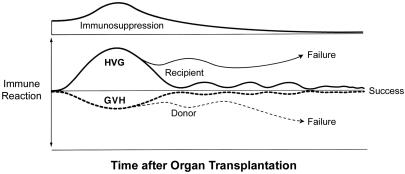
Studies in experimental models (1953-1956) demonstrated that acquired donor-specific allotolerance in immunologically immature or irradiated animals is strongly associated with donor leukocyte chimerism. Bone marrow transplantation in immune-deficient or cytoablated human recipients was a logical extension (1968). In contrast, clinical (1959) and then experimental organ transplantation was systematically accomplished in the apparent absence of leukocyte chimerism. Consequently, it was assumed for many years that success with organ and bone marrow transplantation involved fundamentally different mechanisms. With the discovery in 1992 of small numbers of donor leukocytes in the tissues or blood of long-surviving organ recipients (microchimerism), we concluded that organ engraftment was a form of leukocyte chimerism-dependent partial tolerance. In this initially controversial paradigm, alloengraftment after both kinds of transplantation is the product of a double immune reaction in which responses, each to the other, of coexisting donor and recipient immune systems results in variable reciprocal clonal exhaustion, followed by peripheral clonal deletion. It was proposed with Rolf Zinkernagel that the individual alloresponses are the equivalent of the MHC-restricted T cell recognition of, and host response to, intracellular parasites and that the mechanisms of immune responsiveness, or nonresponsiveness, are governed by the migration and localization of the respective antigens. Elucidation of the mechanisms of nonresponsiveness (clonal exhaustion-deletion and immune ignorance) and their regulation removed much of the historical mystique of transplantation. The insight was then applied to improve the timing and dosage of immunosuppression of current human transplant recipients.
Figures
Similar articles
-
The mystique of hepatic tolerogenicity.Semin Liver Dis. 2000;20(4):497-510. doi: 10.1055/s-2000-13158. Semin Liver Dis. 2000. PMID: 11200418 Review.
-
Cellular basis of long-term organ transplant acceptance: pivotal role of intrathymic clonal deletion and thymic dependence of bone marrow microchimerism-associated tolerance.Am J Kidney Dis. 1998 Feb;31(2):197-212. doi: 10.1053/ajkd.1998.v31.pm9469488. Am J Kidney Dis. 1998. PMID: 9469488 Review.
-
Facilitating cells as a venue to establish mixed chimerism and tolerance.Pediatr Transplant. 2003 Oct;7(5):348-57. doi: 10.1034/j.1399-3046.2003.00100.x. Pediatr Transplant. 2003. PMID: 14738294 Review.
-
The importance of MHC class II in allogeneic bone marrow transplantation and chimerism-based solid organ tolerance in a rat model.PLoS One. 2020 May 22;15(5):e0233497. doi: 10.1371/journal.pone.0233497. eCollection 2020. PLoS One. 2020. PMID: 32442182 Free PMC article.
-
A nonlethal conditioning approach to achieve durable multilineage mixed chimerism and tolerance across major, minor, and hematopoietic histocompatibility barriers.J Immunol. 1995 Nov 1;155(9):4179-88. J Immunol. 1995. PMID: 7594573
Cited by
-
Cell migration from baby to mother.Cell Adh Migr. 2007 Jan-Mar;1(1):19-27. Epub 2007 Jan 28. Cell Adh Migr. 2007. PMID: 19262088 Free PMC article. Review.
-
Acquired immunologic tolerance: with particular reference to transplantation.Immunol Res. 2007;38(1-3):6-41. doi: 10.1007/s12026-007-0001-7. Immunol Res. 2007. PMID: 17917005 Free PMC article.
-
Dichotomy between T Cell and B Cell Tolerance to Neonatal Retroviral Infection Permits T Cell Therapy.J Immunol. 2016 Nov 1;197(9):3628-3638. doi: 10.4049/jimmunol.1600734. Epub 2016 Sep 19. J Immunol. 2016. PMID: 27647833 Free PMC article.
-
Donor-derived peripheral mononuclear cell DNA is associated with stable kidney allograft function: a randomized controlled trial.Chimerism. 2011 Oct-Dec;2(4):102-10. doi: 10.4161/chim.2.4.19095. Chimerism. 2011. PMID: 22509426 Free PMC article. Clinical Trial.
-
Harnessing Expressed Single Nucleotide Variation and Single Cell RNA Sequencing To Define Immune Cell Chimerism in the Rejecting Kidney Transplant.J Am Soc Nephrol. 2020 Sep;31(9):1977-1986. doi: 10.1681/ASN.2020030326. Epub 2020 Jul 15. J Am Soc Nephrol. 2020. PMID: 32669324 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
