

Thromboembolism after trauma: an analysis of 1602 episodes from the American College of Surgeons National Trauma Data Bank
- PMID: 15319720
- PMCID: PMC1356439
- DOI: 10.1097/01.sla.0000137138.40116.6c
Thromboembolism after trauma: an analysis of 1602 episodes from the American College of Surgeons National Trauma Data Bank
Abstract
Objective: Venous thromboembolic events (VTE) are potentially preventable causes of morbidity and mortality after injury. We hypothesized that the current clinical incidence of VTE is relatively low and that VTE risk factors could be identified.
Methods: We queried the ACS National Trauma Data Bank for episodes of deep venous thrombosis (DVT) and/or pulmonary embolism (PE). We examined demographic data, VTE risk factors, outcomes, and VTE prophylaxis measures in patients admitted to the 131 contributing trauma centers.
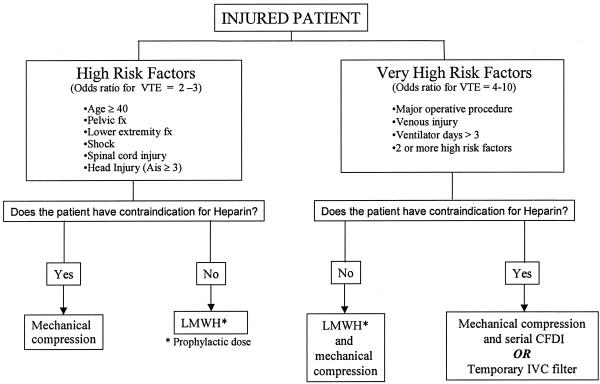
Results: From a total of 450,375 patients, 1602 (0.36%) had a VTE (998 DVT, 522 PE, 82 both), for an incidence of 0.36%. Ninety percent of patients with VTE had 1 of the 9 risk factors commonly associated with VTE. Six risk factors found to be independently significant in multivariate logistic regression for VTE were age > or = 40 years (odds ratio [OR] 2.01; 95% confidence interval [CI] 1.74 to 2.32), lower extremity fracture with AIS > or = 3 (OR 1.92; 95% CI 1.64 to 2.26), head injury with AIS > or = 3 (OR 1.24; 95% CI 1.05 to 1.46), ventilator days >3 (OR 8.08; 95% CI 6.86 to 9.52), venous injury (OR 3.56; 95% CI 2.22 to 5.72), and a major operative procedure (OR 1.53; 95% CI 1.30 to 1.80). Vena cava filters were placed in 3,883 patients, 86% as PE prophylaxis, including in 410 patients without an identifiable risk factor for VTE.
Conclusions: Patients who need VTE prophylaxis after trauma can be identified based on risk factors. The use of prophylactic vena cava filters should be re-examined.
Figures
References
-
- Knudson MM, Collins JA, Goodman SB, et al. Thromboembolism following multiple trauma. J Trauma. 1992;92:2–11. - PubMed
-
- Knudson MM, Lewis FR, Clinton A, et al. Prevention of venous thromboembolism in trauma patients. J Trauma. 1994;97:480–487. - PubMed
-
- Rogers FB. Venous thromboembolism in trauma patients: a review. Surgery. 2001;130:1–12. - PubMed
-
- Geerts WH, Code KI, Jay RM, et al. A prospective study of venous thromboembolism after major trauma. N Engl J Med. 1994;331:1601–1606. - PubMed
-
- Shackford SR, Davis JW, Hollingsworth-Frielund P, et al. Venous thromboembolism in patients with major trauma. Am J Surg. 1990;159:365–369. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
