

Carotid endarterectomy at the millennium: what interventional therapy must match
- PMID: 15319725
- PMCID: PMC1356444
- DOI: 10.1097/01.sla.0000137142.26925.3c
Carotid endarterectomy at the millennium: what interventional therapy must match
Abstract
Objectives: Carotid endarterectomy (CEA) is supported by level 1 evidence as the standard treatment of severe carotid stenosis in both symptomatic and asymptomatic patients. As interventional techniques are emerging for treatment of this disease, this study was undertaken to provide a contemporary surgical standard for comparison to carotid stenting.
Patients and methods: During the interval 1989 to 1999, 2236 isolated CEAs were performed on 1897 patients (62% male, 36% symptomatic, 4.6% reoperative procedures). Study endpoints included perioperative events, patient survival, late incidence of stroke, anatomic durability of CEA, and resource utilization changes during the study. Variables associated with complications, long-term and stroke free survival, restenosis, and resource utilization were analyzed by univariate and multivariate analysis.
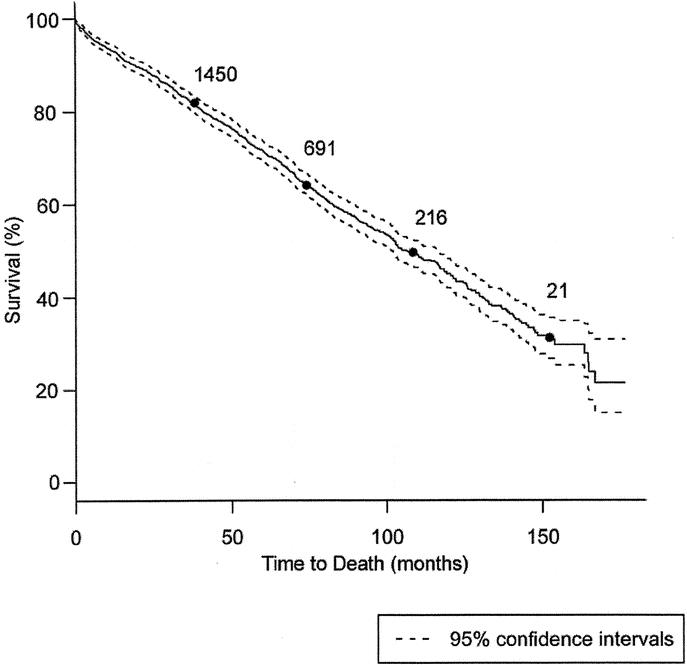
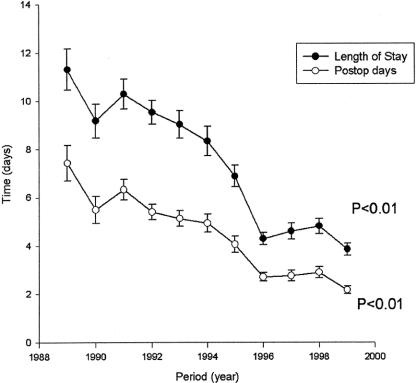
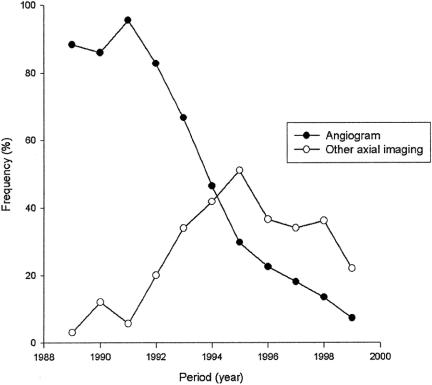
Results: Perioperative complications occurred in 5.5% of CEA procedures, including any stroke/death (1.4%), neck hematoma (1.7%), cardiac complications (0.5%), and cranial nerve injury (0.4%). Actuarial survival at 5 and 10 years was 72.4% (95% confidence interval [CI] 69.3-73.5) and 44.7% (95% CI 41.7-47.9) respectively, with coronary artery disease (P < 0.0018), chronic obstructive pulmonary disease (P < 0.00018) and diabetes mellitus (P < 0.0011) correlating with decreased longevity. The age- and sex-adjusted incidence of any stroke during follow-up was reduced by 22% (upper 0.35, lower 0.08) of predicted with the patient classification of hyperlipidemia (P < 0.0045) as the only protective factor. Analysis of CEA anatomic durability during a median follow-up period of 5.9 years identified a 7.7% failure rate (severe restenosis/occlusion, 4.5%; or reoperative CEA, 3.2%) with elevated serum cholesterol (P < 0.017) correlating with early restenosis. Resource utilization diminished (first versus last 2-year interval periods) for average hospital length of stay from 10.3 +/- 1.5 days to 4.3 +/- 0.7 days (P < 0.01) and preoperative contrast angiography from 87% +/- 1.4% to 10.3% +/- 4%.
Conclusions: These data delineate the safety, durability, and effectiveness in long-term stroke prevention of CEA. They provide a standard to which emerging catheter-based therapies for carotid stenosis should be compared.
Figures
Similar articles
-
Determinants of carotid endarterectomy anatomic durability: effects of serum lipids and lipid-lowering drugs.J Vasc Surg. 2005 May;41(5):762-8. doi: 10.1016/j.jvs.2005.01.035. J Vasc Surg. 2005. PMID: 15886657
-
Carotid artery stenting outcomes are equivalent to carotid endarterectomy outcomes for patients with post-carotid endarterectomy stenosis.J Vasc Surg. 2010 Nov;52(5):1180-7. doi: 10.1016/j.jvs.2010.06.074. Epub 2010 Aug 8. J Vasc Surg. 2010. PMID: 20692794
-
Stenting versus endarterectomy after prior ipsilateral carotid endarterectomy.J Vasc Surg. 2017 Jan;65(1):1-11. doi: 10.1016/j.jvs.2016.07.115. Epub 2016 Oct 1. J Vasc Surg. 2017. PMID: 27707617
-
Meta-analysis of redo stenting versus endarterectomy for in-stent stenosis after carotid artery stenting.J Vasc Surg. 2021 Apr;73(4):1282-1289. doi: 10.1016/j.jvs.2020.07.102. Epub 2020 Aug 28. J Vasc Surg. 2021. PMID: 32861870
-
Endarterectomy or carotid artery stenting: the quest continues.Am J Surg. 2008 Feb;195(2):259-69. doi: 10.1016/j.amjsurg.2007.07.022. Am J Surg. 2008. PMID: 18154764 Review.
Cited by
-
Risk Factors of Cerebral Infarction and Myocardial Infarction after Carotid Endarterectomy Analyzed by Machine Learning.Comput Math Methods Med. 2020 Nov 12;2020:6217392. doi: 10.1155/2020/6217392. eCollection 2020. Comput Math Methods Med. 2020. PMID: 33273961 Free PMC article.
-
Revitalizing neurosurgical frontiers: The EANS frontiers in neurosurgery committee's strategic framework.Brain Spine. 2024 Mar 26;4:102794. doi: 10.1016/j.bas.2024.102794. eCollection 2024. Brain Spine. 2024. PMID: 38601776 Free PMC article.
-
Carotid stenting done exclusively by vascular surgeons: first 175 cases.Ann Surg. 2005 Sep;242(3):431-6; discussion 436-8. doi: 10.1097/01.sla.0000179650.89508.2f. Ann Surg. 2005. PMID: 16135929 Free PMC article.
-
Protamine reduces bleeding complications associated with carotid endarterectomy without increasing the risk of stroke.J Vasc Surg. 2010 Mar;51(3):559-64, 564.e1. doi: 10.1016/j.jvs.2009.10.078. Epub 2010 Jan 4. J Vasc Surg. 2010. PMID: 20045609 Free PMC article.
-
Association of Transcarotid Artery Revascularization vs Transfemoral Carotid Artery Stenting With Stroke or Death Among Patients With Carotid Artery Stenosis.JAMA. 2019 Dec 17;322(23):2313-2322. doi: 10.1001/jama.2019.18441. JAMA. 2019. PMID: 31846015 Free PMC article.
References
-
- North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991;325:445–453. - PubMed
-
- Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351:1379–1387. - PubMed
-
- Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. Endarterectomy for asymptomatic carotid artery stenosis. JAMA. 1995;273:1421–1428. - PubMed
-
- Moore WS, Barnett HJ, Beebe HG, et al. Guidelines for carotid endarterectomy: a multidisciplinary consensus statement from the Ad Hoc Committee, American Heart Association. Circulation. 1995;91:566–579. - PubMed
-
- Anthony T, Johansen K. Optimal outcome for “high-risk” carotid endarterectomy. Am J Surg. 1994;167:469–471. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
