

Predicting outcome in ex-premature infants supported with extracorporeal membrane oxygenation for acute hypoxic respiratory failure
- PMID: 15321962
- PMCID: PMC1721757
- DOI: 10.1136/adc.2003.033308
Predicting outcome in ex-premature infants supported with extracorporeal membrane oxygenation for acute hypoxic respiratory failure
Abstract
Objective: To identify predictors of outcome in ex-premature infants supported with extracorporeal membrane oxygenation (ECMO) for acute hypoxic respiratory failure.
Methods: Retrospective review of ex-premature infants with acquired acute hypoxic respiratory failure requiring ECMO support in the United Kingdom from 1992 to 2001. Review of follow up questionnaires completed by general practitioners and local paediatricians.
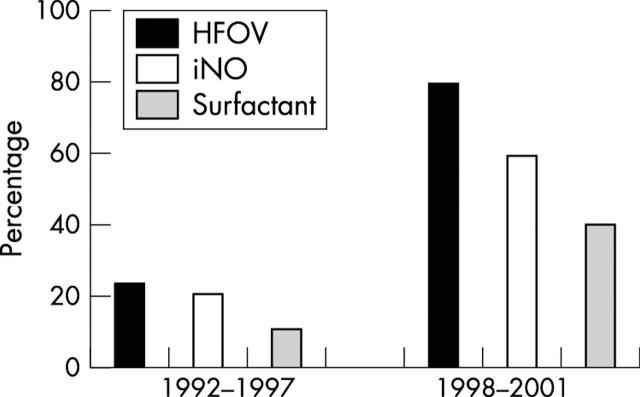
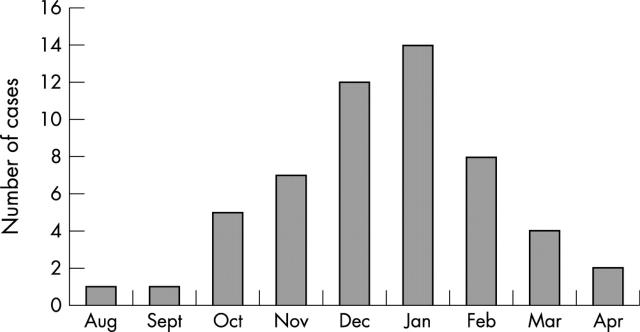
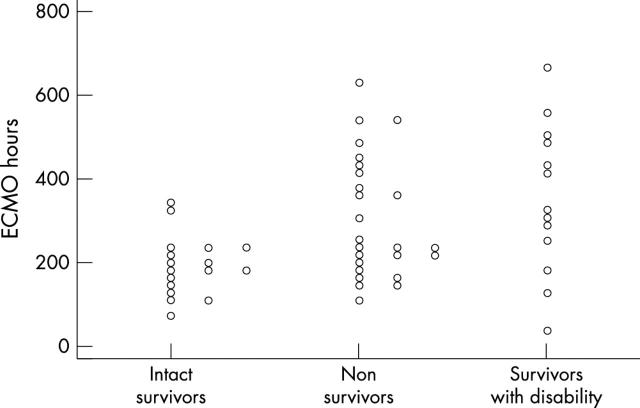
Results: Sixty four ex-premature infants (5-10 each year) received ECMO support, despite increased use of advanced conventional treatments over the decade. The most common infective agent was respiratory syncytial virus (85% of cases). Median birth gestation was 29 weeks and median corrected age at the time of ECMO support was 42 weeks. Median ECMO support duration was relatively long, at 229 hours. Survival to hospital discharge and to 6 months was 80%, remaining similar throughout the period of review. At follow up, 60% had long term neurodisability and 79% had chronic pulmonary problems. Of pre-ECMO factors, baseline oxygen dependence, younger age, and inpatient status were associated with non-survival (p < or = 0.05). Of ECMO related factors, patient complications were independently associated with adverse neurodevelopmental outcome and death (p < 0.01).
Conclusions: Survival rates for ex-premature infants after ECMO support are favourable, but patients suffer a high burden of morbidity during intensive care and over the long term. At the time of ECMO referral, baseline oxygen dependence is the most important predictor of death, but no combination of the factors considered was associated with a mortality that would preclude ECMO support.
Figures
Similar articles
-
Survivors of extracorporeal membrane oxygenation at 1 year of age: the relationship of primary diagnosis with health and neurodevelopmental sequelae.Pediatrics. 1995 Nov;96(5 Pt 1):907-13. Pediatrics. 1995. PMID: 7478834
-
Primary use of the venovenous approach for extracorporeal membrane oxygenation in pediatric acute respiratory failure.Pediatr Crit Care Med. 2003 Jul;4(3):291-8. doi: 10.1097/01.PCC.0000074261.09027.E1. Pediatr Crit Care Med. 2003. PMID: 12831409
-
Extracorporeal membrane oxygenation in infants with meconium aspiration syndrome: a decade of experience with venovenous ECMO.J Pediatr Surg. 2005 Jul;40(7):1082-9. doi: 10.1016/j.jpedsurg.2005.03.045. J Pediatr Surg. 2005. PMID: 16034749
-
Factors associated with sensorineural hearing loss among survivors of extracorporeal membrane oxygenation therapy.Pediatrics. 2005 Jun;115(6):1519-28. doi: 10.1542/peds.2004-0247. Pediatrics. 2005. PMID: 15930212 Review.
-
Respiratory failure and extracorporeal membrane oxygenation.Semin Pediatr Surg. 2008 Feb;17(1):34-41. doi: 10.1053/j.sempedsurg.2007.10.006. Semin Pediatr Surg. 2008. PMID: 18158140 Review.
Cited by
-
Predictors of outcome for children requiring respiratory extra-corporeal life support: implications for inclusion and exclusion criteria.Intensive Care Med. 2008 Dec;34(12):2256-63. doi: 10.1007/s00134-008-1232-3. Epub 2008 Aug 1. Intensive Care Med. 2008. PMID: 18670760
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical