

Control of frontal plane knee laxity during gait in patients with medial compartment knee osteoarthritis
- PMID: 15325641
- PMCID: PMC3123521
- DOI: 10.1016/j.joca.2004.05.005
Control of frontal plane knee laxity during gait in patients with medial compartment knee osteoarthritis
Abstract
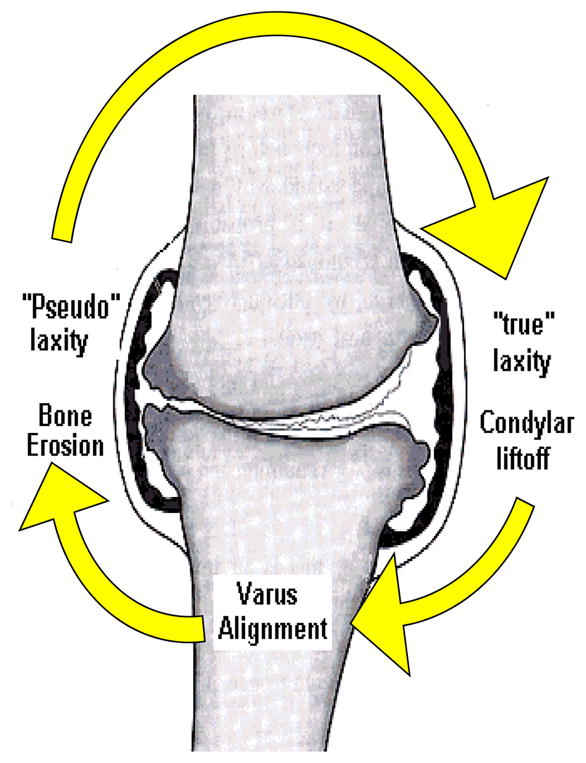
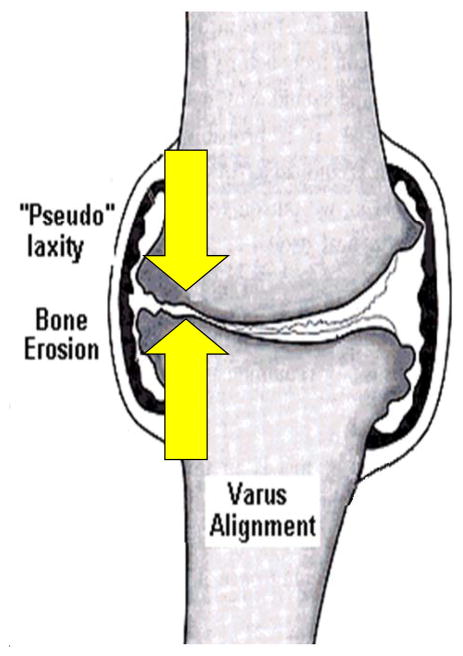
Objective: Patients with medial compartment knee osteoarthritis (OA) adopt an abnormal gait pattern, and often develop frontal plane laxity at the knee. The purpose of this study was to quantify the extent of frontal plane knee joint laxity in patients with medial knee OA and genu varum and to assess the effect of joint laxity on knee joint kinetics, kinematics and muscle activity during gait.
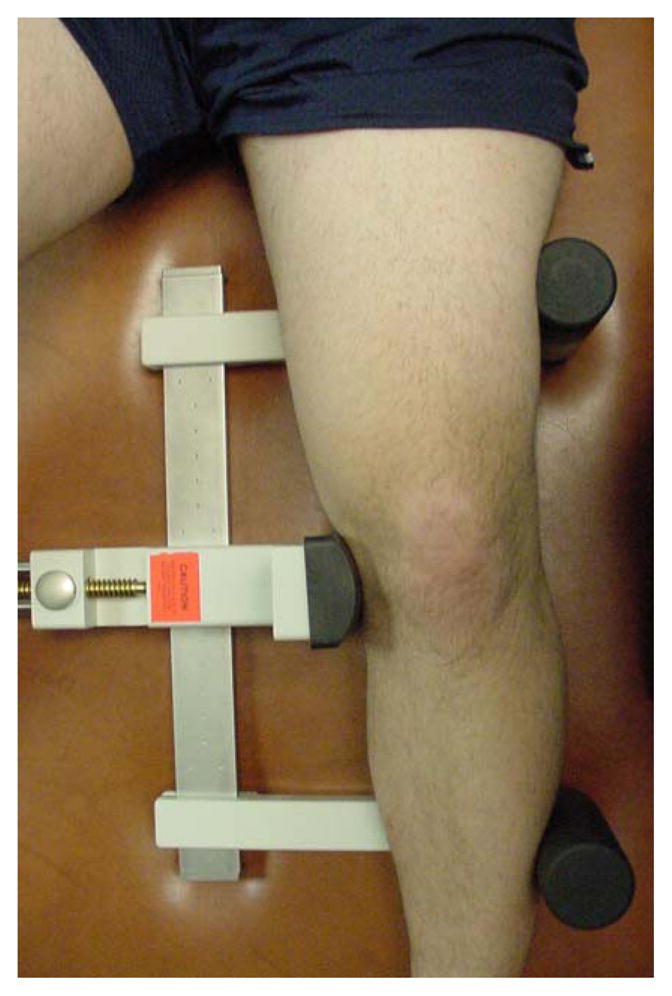
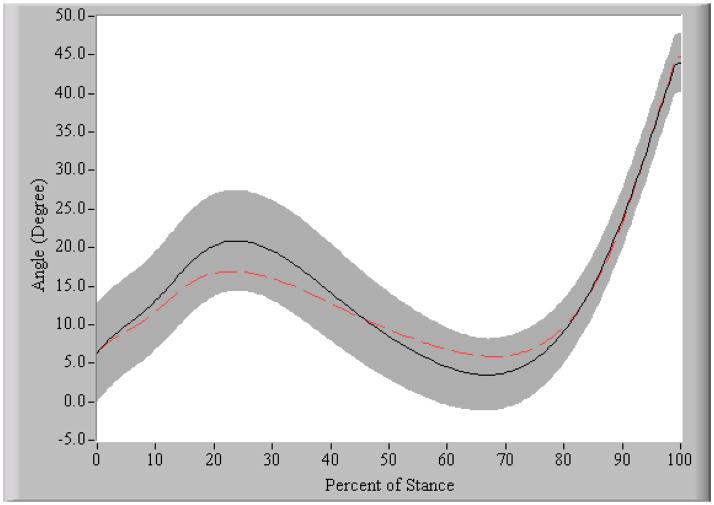
Design: Twelve subjects with genu varum and medial compartment knee osteoarthritis (OA group) and 12 age-matched uninjured subjects underwent stress radiography to determine the presence and magnitude of frontal plane laxity. All subjects also went through gait analysis with surface electromyography of the medial and lateral quadriceps, hamstrings, and gastrocnemius to calculate knee joint kinematics and kinetics and co-contraction levels during gait.
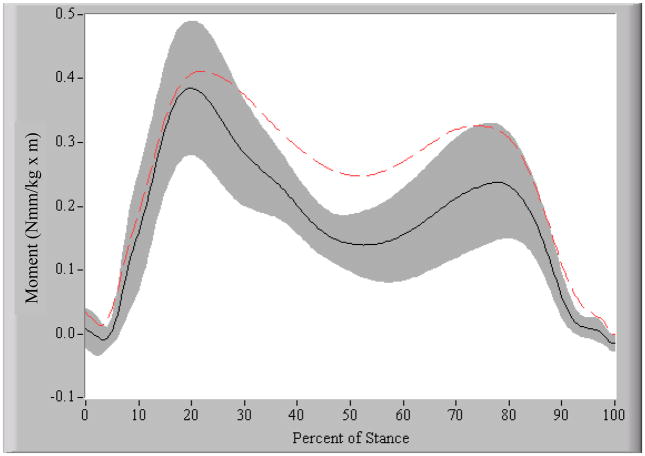
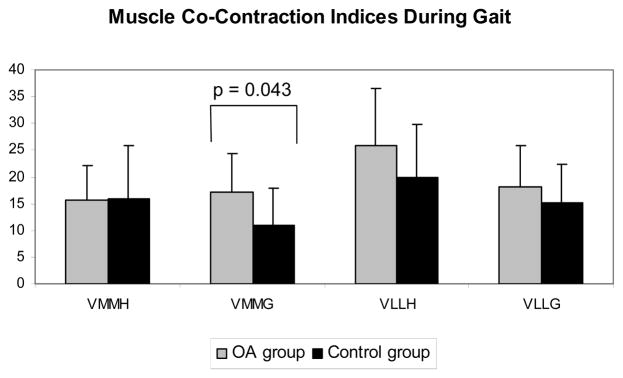
Results: The OA group showed significantly greater knee instability (P = 0.002), medial joint laxity (P = 0.001), greater medial quadriceps-medial gastrocnemius (VMMG) co-contraction (P = 0.043), and greater knee adduction moments (P = 0.019) than the control group. Medial joint laxity contributed significantly to the variance in both VMMG and the knee adduction moment during early stance.
Conclusion: The presence of medial laxity in patients with knee OA is likely contributing to the altered gait patterns observed in those with medial knee OA. Greater medial co-contraction and knee adduction moments bodes poorly for the long-term integrity of the articular cartilage, suggesting that medial joint laxity should be a focus of interventions aimed at slowing the progression of disease in individuals with medial compartment knee OA.
Figures
References
-
- Dearborn JT, Eakin CL, Skinner HB. Medial compartment arthrosis of the knee. Am J Orthop. 1996;25(1):18–26. - PubMed
-
- Bartel DL. Unicompartmental arthritis: biomechanics and treatment alternatives. Instr Course Lect. 1992;41:73–6. - PubMed
-
- Wu DD, Burr DB, Boyd RD, Radin EL. Bone and cartilage changes following experimental varus or valgus tibial angulation. J Orthop Res. 1990;8(4):572–85. - PubMed
-
- Sharma L, Song J, Felson DT, Cahue S, Shamiyeh E, Dunlop DD. The role of knee alignment in disease progression and functional decline in knee osteoarthritis. Jama. 2001;286(2):188–95. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
