

Is intraoperative electrocorticography reliable in children with intractable neocortical epilepsy?
- PMID: 15329074
- PMCID: PMC1829315
- DOI: 10.1111/j.0013-9580.2004.65803.x
Is intraoperative electrocorticography reliable in children with intractable neocortical epilepsy?
Abstract
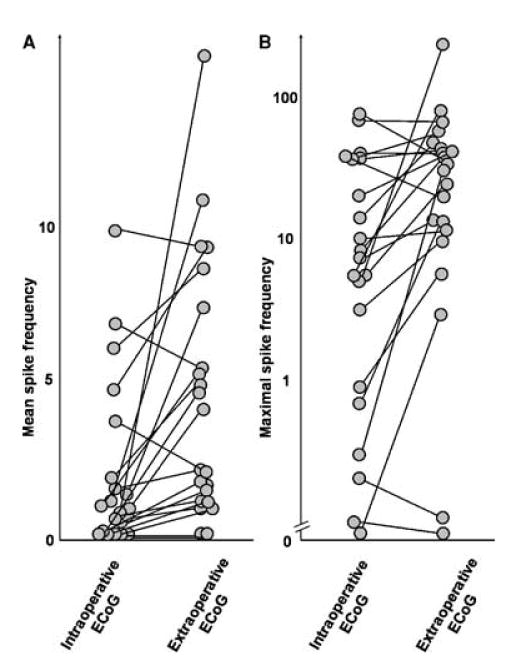
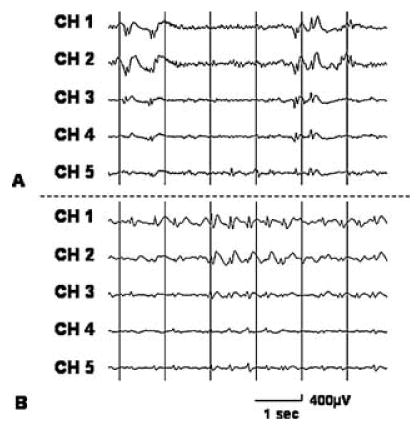
Purpose: To study the relation between the spike frequency during intraoperative electrocorticography (ECoG) under general anesthesia with isoflurane and that during extraoperative ECoG monitoring in children with intractable neocortical epilepsy.
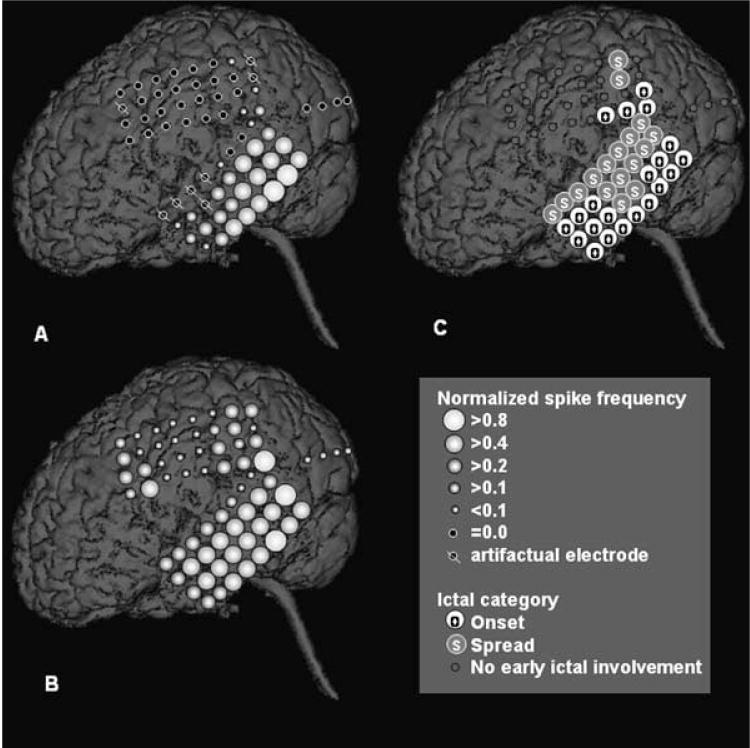
Methods: Twenty-one children (age, 1-16 years; 15 boys and six girls) who underwent intraoperative and extraoperative ECoG monitoring with subdural electrode arrays were studied. The spike frequency and the spatial pattern of spike frequency were compared between intraoperative and extraoperative ECoGs for each patient (by using Wilcoxon signed-ranks and Spearman's rank correlation, respectively).
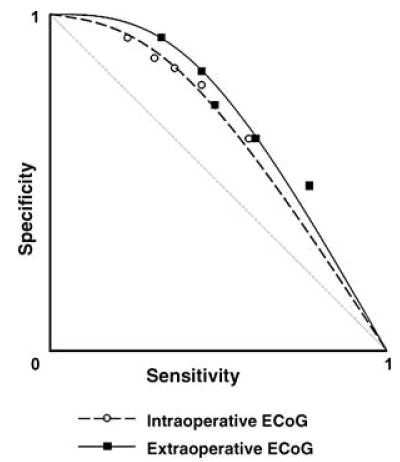
Results: In 15 of 21 patients, the spike frequency was significantly lower during intraoperative than during extraoperative ECoG (mean z = -6.3; p < 0.001). In four of 21 patients, no significant difference was found in the spike frequency between intraoperative and extraoperative recordings. In two of 21 patients, spike frequency reached one spike/min neither during intraoperative nor extraoperative recording; therefore appropriate comparison of spike frequency was not possible. A significant positive correlation in the spike-frequency pattern was seen between intraoperative and extraoperative recordings in nine of nine cases who had > or = 10 spikes/min during intraoperative ECoG (mean rho = 0.62; p < 0.01), in five of six cases with one to nine spikes/min (mean rho = 0.50; p < 0.01), and in none of five cases with less than one spike/min (mean rho = 0.13).
Conclusions: General anesthesia often decreases the spike frequency in children with neocortical epilepsy, yet intraoperative ECoG can reliably reflect the awake interictal spiking pattern when spike frequency exceeds one spike/min during intraoperative ECoG recording.
Copyright 2004 International League Against Epilepsy
Figures
References
-
- Luders HO, Engel J, Jr, Munari C. General Principles. In: Engel J Jr, editor. Surgical treatment of epilepsies. 1993. 2nd ed. New York: Raven Press; pp. 137–53.
-
- Keene DL, Whiting S, Ventureyra EC. Electrocorticography. Epileptic Disord. 2000;2:57–63. - PubMed
-
- Onal C, Otsubo H, Araki T, et al. Complications of invasive subdural grid monitoring in children with epilepsy. J Neurosurg. 2003;98:1017–26. - PubMed
-
- Fiol ME, Boening JA, Cruz-Rodriguez R, et al. Effect of isoflurane (Forane) on intraoperative electrocorticogram. Epilepsia. 1993;34:897–900. - PubMed
-
- Ito BM, Sato S, Kufta CV, et al. Effect of isoflurane and enflurane on the electrocorticogram of epileptic patients. Neurology. 1988;38:924–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
