

Efficacy of interventions for bronchiolitis in critically ill infants: a systematic review and meta-analysis
- PMID: 15329166
- PMCID: PMC3867796
- DOI: 10.1097/01.pcc.0000128891.54799.67
Efficacy of interventions for bronchiolitis in critically ill infants: a systematic review and meta-analysis
Abstract
Background: Viral bronchiolitis is the leading cause of respiratory failure among infants in the United States. Currently, the mainstay of treatment is supportive care. The effectiveness of treatments used for mechanically ventilated infants with bronchiolitis is unclear.
Objective: To evaluate the strength of the evidence supporting the use of currently available treatments for critically ill infants with bronchiolitis.
Data source: We searched PubMed, citations of relevant articles, personal files, and conference proceedings, and we contacted experts in the field.
Study selection: Randomized, controlled trials evaluating any therapy for bronchiolitis that included children in an intensive care unit.
Data extraction: Two reviewers independently extracted data and assessed methodologic quality.
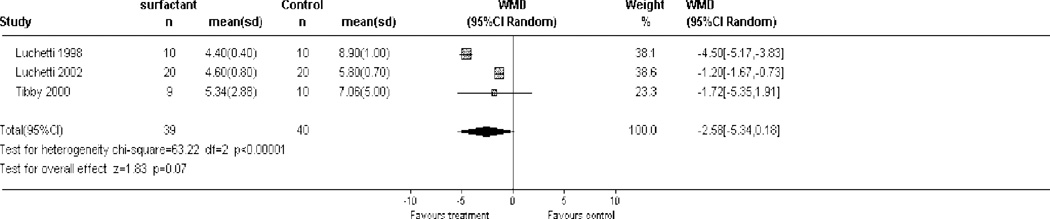
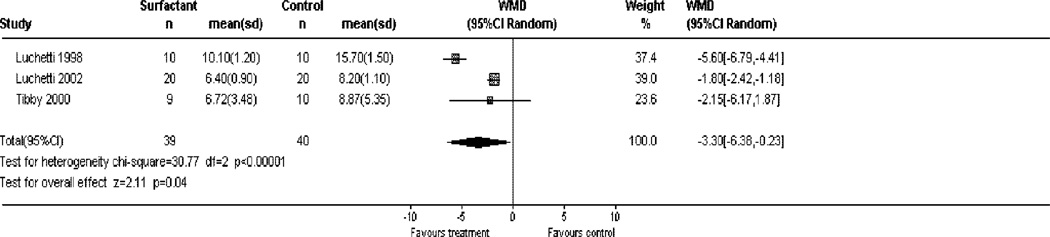
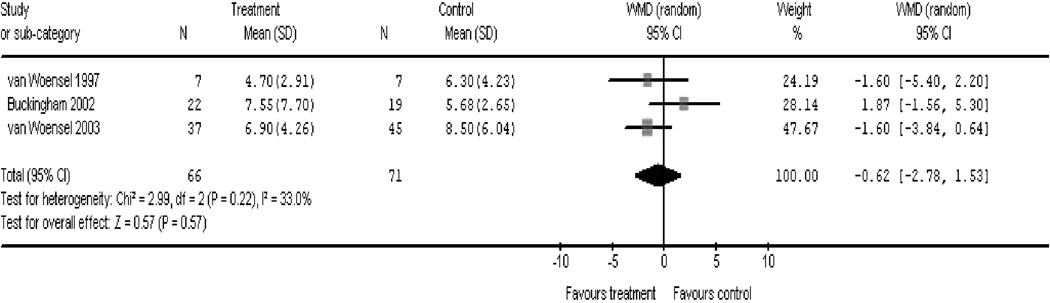
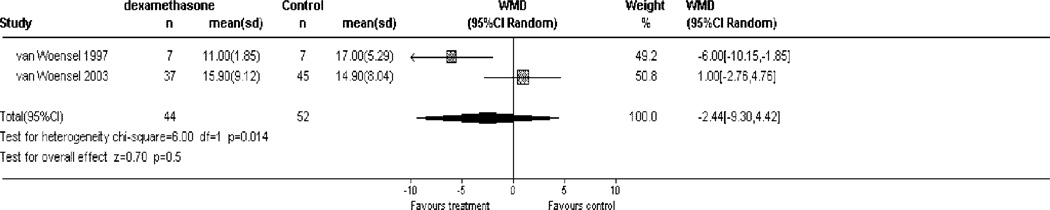
Data synthesis: A total of 2,319 citations were screened, and 16 randomized, controlled trials were included. There were three trials of surfactant, three of ribavirin, three of immune globulin, three of systemic corticosteroids, and one each of vitamin A, interferon, erythropoietin, and heliox. A meta-analysis of the three surfactant studies showed a strong trend toward a decrease in duration of mechanical ventilation of 2.58 days (95% confidence interval, -5.34 to 0.18 days; p =.07) and a significant decrease of 3.3 intensive care unit days (95% confidence interval, -6.38 to -0.23 days; p =.04). A meta-analysis of the three systemic corticosteroid studies showed no overall effect on duration of mechanical ventilation when all three trials were combined (-0.62 day; 95% confidence interval, -2.78 to 1.53 days; p =.57). We identified one published meta-analysis of three ribavirin studies showing a significant decrease in ventilator days with ribavirin (-1.2 days; 95% confidence interval, -0.2 to -3.4 days; p =.2).
Conclusions: Currently, there are no clearly effective interventions available to improve the outcome of critically ill infants with bronchiolitis. Surfactant seems to be a promising intervention, and corticosteroids or ribavirin may also be beneficial.
Figures
Comment in
-
Bronchiolitis: what's next?Pediatr Crit Care Med. 2004 Sep;5(5):498-500. doi: 10.1097/01.pcc.0000130991.23217.88. Pediatr Crit Care Med. 2004. PMID: 15356398 No abstract available.
References
-
- Law BJ, De Carvalho V. Respiratory syncytial virus infections in hospitalized Canadian children: Regional differences in patient populations and management practices. The Pediatric Investigators Collaborative Network on Infections in Canada. Pediatr Infect Dis J. 1993;12:659–663. - PubMed
-
- Hall CB. Respiratory syncytial virus and parainfluenza virus. N Engl J Med. 2001;344:1917–1928. - PubMed
-
- Shay DK, Holman RC, Newman RD, et al. Bronchiolitis-associated hospitalizations among US children, 1980–1996. JAMA. 1999;282:1440–1446. - PubMed
-
- Navas L, Wang E, de Carvalho V, et al. Improved outcome of respiratory syncytial virus infection in a high-risk hospitalized population of Canadian children: Pediatric Investigators Collaborative Network on Infections in Canada. J Pediatr. 1992;121:348–354. - PubMed
-
- Buckingham SC, Quasney MW, Bush AJ, et al. Respiratory syncytial virus infections in the pediatric intensive care unit: Clinical characteristics and risk factors for adverse outcomes. Pediatr Crit Care Med. 2001;2:318–323. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
