

Combination of contrast with stress echocardiography: a practical guide to methods and interpretation
- PMID: 15331015
- PMCID: PMC516786
- DOI: 10.1186/1476-7120-2-15
Combination of contrast with stress echocardiography: a practical guide to methods and interpretation
Abstract
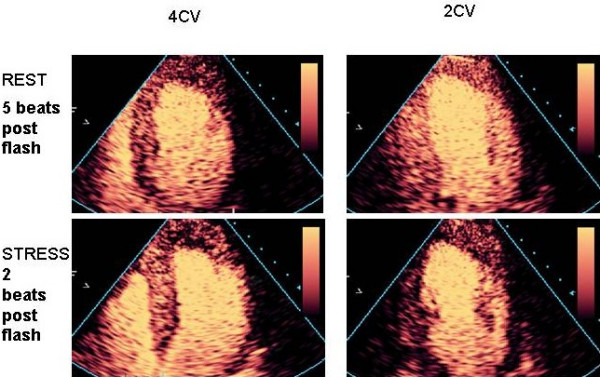
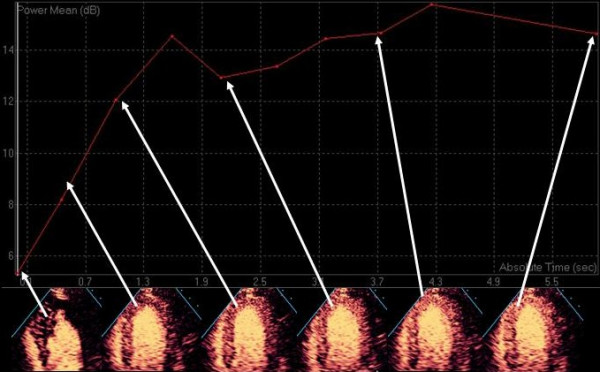
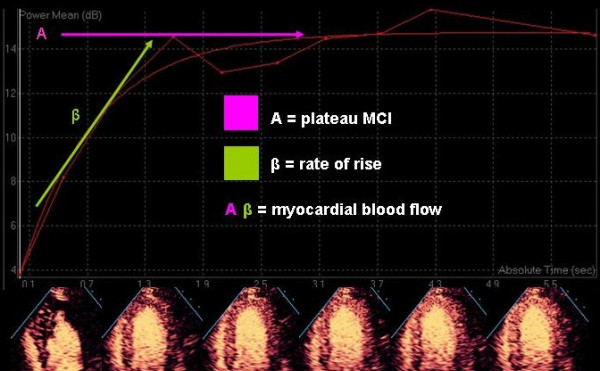
Contrast echocardiography has an established role for enhancement of the right heart Doppler signals, the detection of intra-cardiac shunts, and most recently for left ventricular cavity opacification (LVO). The use of intravenously administered micro-bubbles to traverse the myocardial microcirculation in order to outline myocardial viability and perfusion has been the source of research studies for a number of years. Despite the enthusiasm of investigators, myocardial contrast echocardiography (MCE) has not attained routine clinical use and LV opacification during stress has been less widely adopted than the data would support. The purpose of this review is to facilitate an understanding of the involved imaging technologies that have made this technique more feasible for clinical practice, and to guide its introduction into the practice of the non-expert user.
Figures


References
-
- Reisner SA, Ong LS, Lichtenberg GS, et al. Myocardial perfusion imaging by contrast echocardiography with use of intracoronary sonicated albumin in humans. J Am Coll Cardiol. 1989;14:660–665. - PubMed
-
- Vandenberg BF, Feinstein SB, Kieso RA, Hunt M, Kerber RE. Myocardial risk area and peak gray level measurement by contrast echocardiography: effect of microbubble size and concentration, injection rate, and coronary vasodilation. Am Heart J. 1988;115:733–739. doi: 10.1016/0002-8703(88)90872-1. - DOI - PubMed
-
- Burns PN. Harmonic imaging with ultrasound contrast agents. Clin Radiol. 1996;51:50–55. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
