

Microlaparoscopic-assisted vaginal hysterectomy in the morbidly obese patient
- PMID: 15347109
- PMCID: PMC3016807
Microlaparoscopic-assisted vaginal hysterectomy in the morbidly obese patient
Abstract
Objective: The purpose of this study was to demonstrate a minimally invasive, novel variation, microlaparoscopic-assisted vaginal hysterectomy (MAVH) of a previously established technique, laparoscopic-assisted vaginal hysterectomy (LAVH), in the morbidly obese patient.
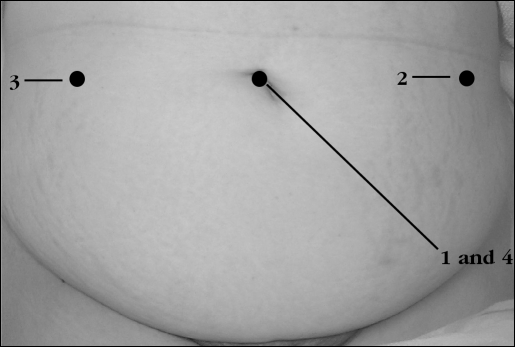
Methods: This was a prospective, descriptive feasibility study (Canadian Task Force classification 11-2) conducted at a university-affiliated hospital and private community hospital. Seven morbidly obese women with an average body mass index of 45.8 kg/m2 (range, 40.6 to 51.5) underwent microlaparoscopic-assisted vaginal hysterectomy (MAVH). Microlaparoscopic-assisted vaginal hysterectomy (MAVH), classified as Type 1B, including unilateral or bilateral occlusion and division of the ovarian artery(ies), either medial or lateral to the ovary(ies), with or without dissection of the adjacent broad ligament under microlaparoscopic guidance, in addition to incision of the vesicouterine peritoneum.
Results: The median duration of surgery was 109.1 minutes (range, 86 to 134), median blood loss was 207 mL (range, 100 to 350), and average length of stay in the hospital was 33.7 hours (range, 23 to 48). The complication rate was 0%.
Conclusion: Microlaparoscopic-assisted vaginal hysterectomy (MAVH) is a safe and effective, more minimally invasive method of performing laparoscopic hysterectomies in select morbidly obese patients.
Figures
References
-
- Palter SF. Microlaparoscopy under local anesthesia and conscious pain mapping for the diagnosis and management of pelvic pain. Curr Opinion Obstet Gynecol. 1999;11:387–393 - PubMed
-
- Almeida OD, Jr, Val-Gallas JM, Rizk B. Appendectomy under local anaesthesia following conscious pain mapping with micro-laparoscopy. Human Reprod. 1998;13:588–590 - PubMed
-
- Almeida OD., Jr. Microlaparoscopic equipment. In: Almeida OD, Jr., ed. Microlaparoscopy. New York, New York: Wiley-Liss; 2000;11–18
-
- Wolf AM, Colditz GA. Social and economic effects of body weight in the United States. Am J Clin Nutr. 1996;63(S):466S–469S - PubMed
-
- Reich H, DeCaprio J, McGlynn F. Laparoscopic hysterectomy. J Gynecol Surg. 1989;5:213–217
MeSH terms
LinkOut - more resources
Full Text Sources