

The course of C-reactive protein response in untreated upper respiratory tract infection
- PMID: 15353049
- PMCID: PMC1326064
The course of C-reactive protein response in untreated upper respiratory tract infection
Abstract
Background: High C-reactive protein (CRP) values are frequently found in patients with bacterial respiratory infection, and CRP testing has been shown to be useful in differentiating pneumonia from other respiratory infections. Raised CRP values may also be found in viral respiratory infection, and as a result there is a risk that antibiotics may be wrongly prescribed.
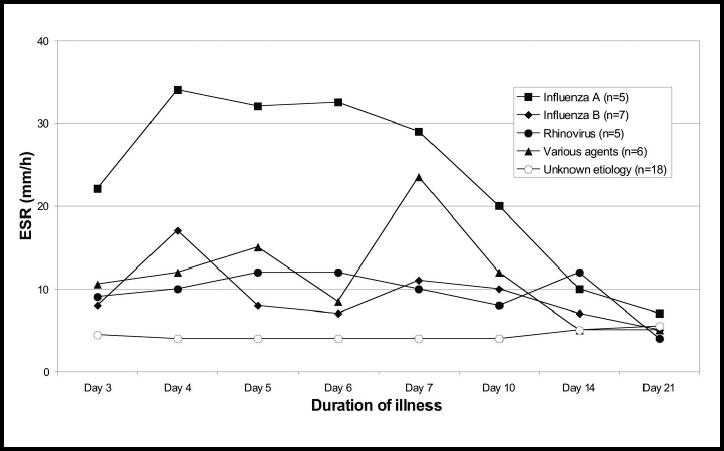
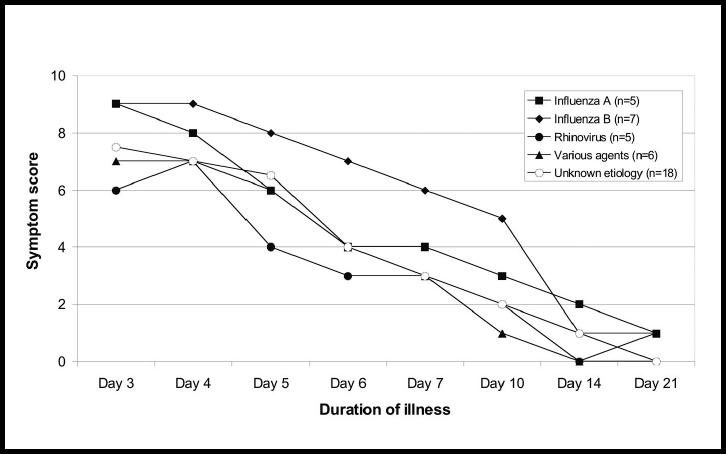
Aims: To describe the course of the CRP response during untreated upper respiratory tract infections and associations between the development of CRP values, erythrocyte sedimentation rate (ESR) and respiratory symptoms.
Design of study: Prospective study.
Setting: Seven general practices in northern Norway.
Method: Patients with upper respiratory tract infection aged 16 years or over, who were not treated with antibiotics and who had been ill for no more than 3 days, were recruited. Microbiological examinations were undertaken, together with measurements of CRP, ESR and recording of symptoms daily during the first week of illness and on days 10, 14 and 21.
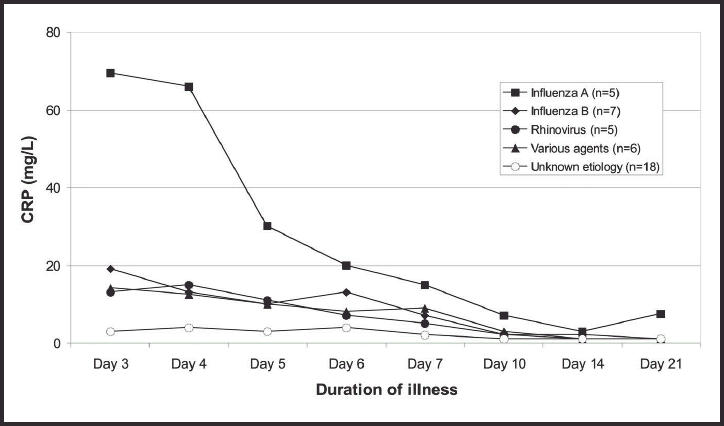
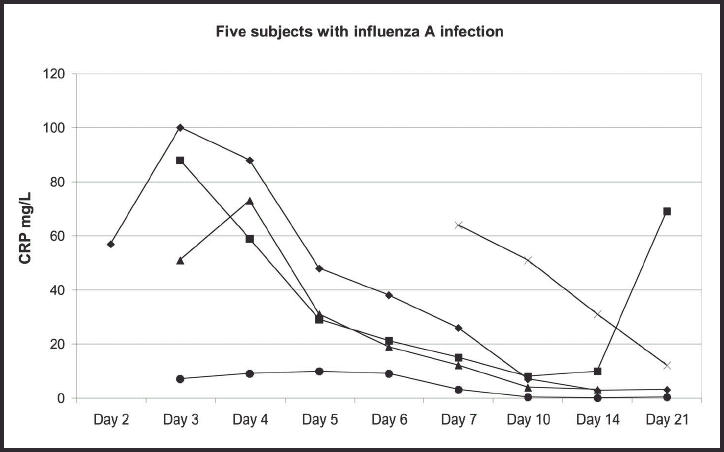
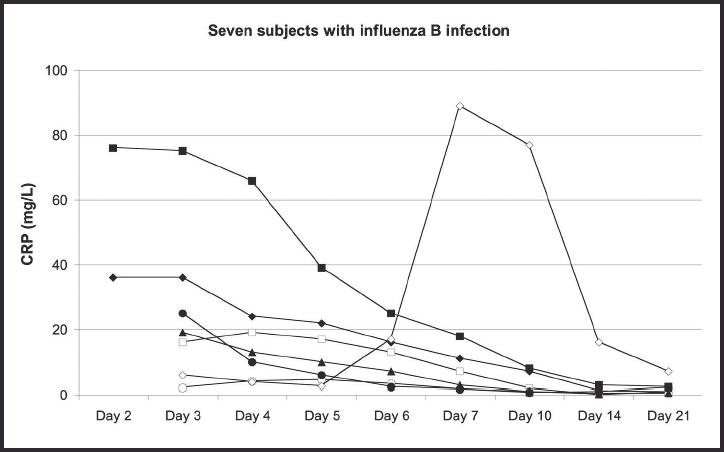
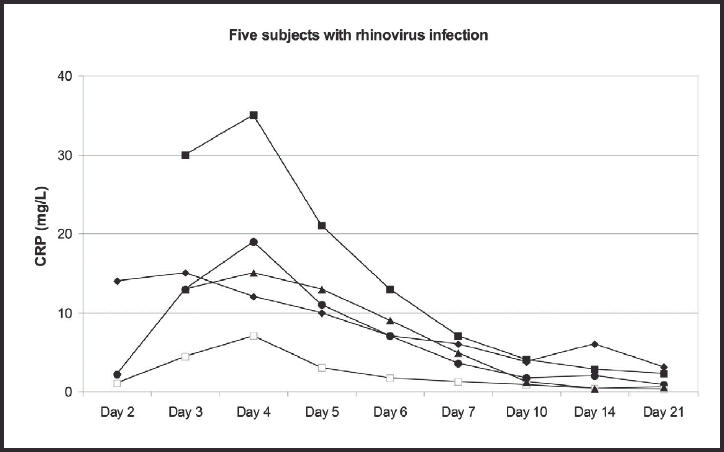
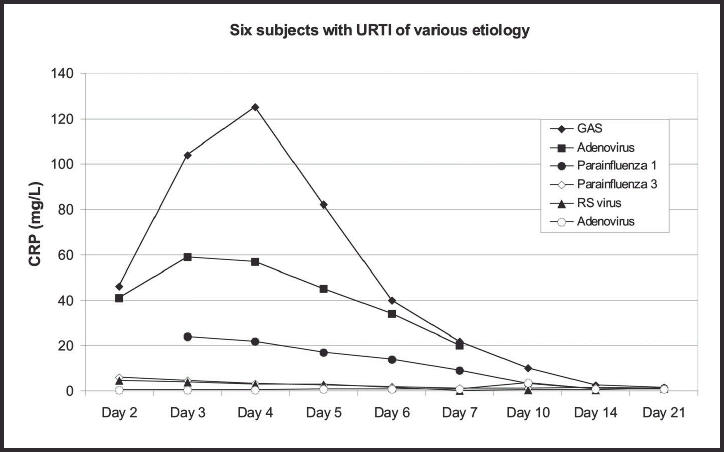
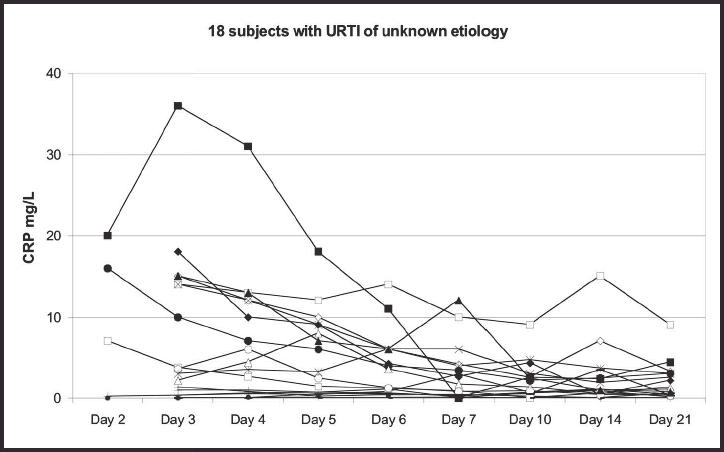
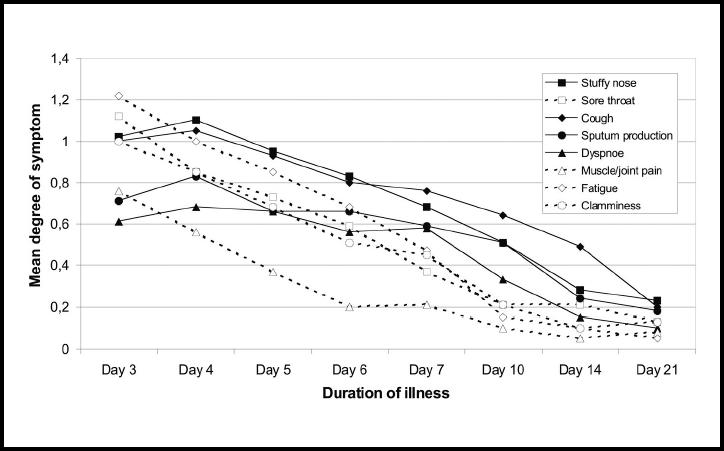
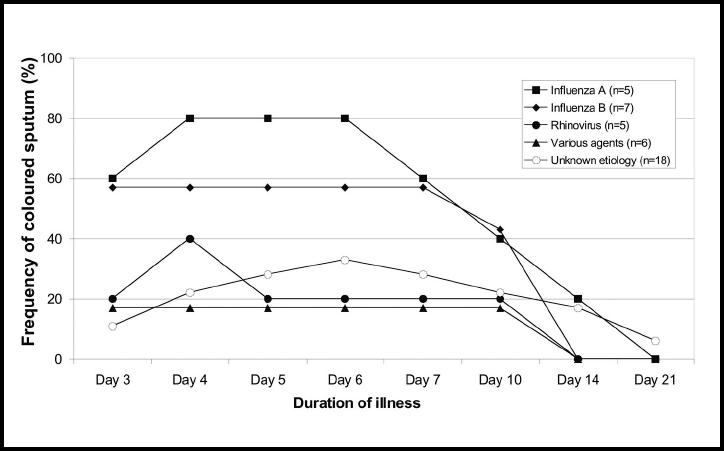
Results: An aetiological agent was established in 23 of the 41 included subjects. These were: influenza A, influenza B, rhinovirus, and other agents. Among the 15 patients examined on both the second and the third day of illness, the median CRP value increased from 7-10 mg/l, and the mean value was from 19-24 mg/l between day 2 and day 3. Peak CRP values were reached on days 2 to 4. Higher CRP values were found in those infected with influenza A and B than in the other subjects (P <0.001). A CRP value >10 mg/l was found in 26 subjects during the first 7 days, compared to five subjects after 1 week. Evidence of a secondary infection with group A streptococci was found in two of these five subjects. The development of the symptoms of sore throat, fatigue, clamminess, and pain from muscles and joints followed a similar course as the CRP response, while stuffy nose, cough, sputum production, and dyspnoea tended to persist after the CRP values had approached the normal range.
Conclusion: A moderately elevated CRP value (10-60 mg/l) is a common finding in viral upper respiratory tract infection, with a peak during days 2-4 of illness. Moderately elevated CRP values cannot support a diagnosis of bacterial infection when the illness has lasted less than 7 days, but may indicate a complication of viral infection after a week.
Figures
Comment in
-
C-reactive protein values in viral respiratory infections.Br J Gen Pract. 2005 Jan;55(510):55. Br J Gen Pract. 2005. PMID: 15667773 Free PMC article. No abstract available.
Similar articles
-
[Evaluation of the usefulness of suction drainage in the treatment of nonspecific bone infections monitored with C-reactive protein].Med Pregl. 1999 Nov-Dec;52(11-12):489-94. Med Pregl. 1999. PMID: 10748773 Clinical Trial. Croatian.
-
Diagnostic utility of CRP to neopterin ratio in patients with acute respiratory tract infections.J Infect. 2009 Feb;58(2):123-30. doi: 10.1016/j.jinf.2008.11.007. Epub 2008 Dec 13. J Infect. 2009. PMID: 19073345
-
C-reactive protein measurement in general practice may lead to lower antibiotic prescribing for sinusitis.Br J Gen Pract. 2004 Sep;54(506):659-62. Br J Gen Pract. 2004. PMID: 15353050 Free PMC article. Clinical Trial.
-
[C-reactive protein in patients with infection].Ugeskr Laeger. 1990 Dec 31;153(1):13-6. Ugeskr Laeger. 1990. PMID: 2275041 Review. Danish.
-
[Diagnostic value of C-reactive protein in bacterial infections. Review of the literature].Ugeskr Laeger. 1998 Aug 17;160(34):4855-9. Ugeskr Laeger. 1998. PMID: 9741250 Review. Danish.
Cited by
-
Clinical characteristics and outcomes of measles outbreak in adults: A multicenter retrospective observational study of 93 hospitalized adults in Greece.J Clin Virol. 2020 Oct;131:104608. doi: 10.1016/j.jcv.2020.104608. Epub 2020 Aug 26. J Clin Virol. 2020. PMID: 32877891 Free PMC article.
-
A pilot study of the use of near-patient C-Reactive Protein testing in the treatment of adult respiratory tract infections in one Irish general practice.BMC Fam Pract. 2011 Aug 31;12:93. doi: 10.1186/1471-2296-12-93. BMC Fam Pract. 2011. PMID: 21880122 Free PMC article.
-
Administering intravenous immunoglobulin during infection is associated with infusion reactions in selected patients.Ir J Med Sci. 2011 Mar;180(1):125-8. doi: 10.1007/s11845-010-0654-4. Epub 2010 Dec 7. Ir J Med Sci. 2011. PMID: 21136195
-
Prevalence and clinical impact of mono- and co-infections with endemic coronaviruses 229E, OC43, NL63, and HKU-1 during the COVID-19 pandemic.Heliyon. 2024 Apr 7;10(7):e29258. doi: 10.1016/j.heliyon.2024.e29258. eCollection 2024 Apr 15. Heliyon. 2024. PMID: 38623185 Free PMC article.
-
Characteristics of hospitalised COVID-19 patients and parameters associated with severe pneumonia.Int J Clin Pract. 2021 Nov;75(11):e14786. doi: 10.1111/ijcp.14786. Epub 2021 Sep 15. Int J Clin Pract. 2021. PMID: 34480831 Free PMC article.
References
-
- André M, Odenholt I, Schwan AM, et al. Upper respiratory tract infections in general practice: diagnosis, antibiotic prescribing, duration of symptoms and use of diagnostic tests. Scand J Infect Dis. 2002;34:880–886. - PubMed
-
- Honkanen PO, Rautakorpi UM, Huovinen P, et al. Diagnostic tools in respiratory tract infections: use and comparison with Finnish guidelines. Scand J Infect Dis. 2002;34:827–830. - PubMed
-
- Hansson LO, Hedlund JU, Ortqvist AB. Sequential changes of inflammatory and nutritional markers in patients with community-acquired pneumonia. Scand J Clin Lab Invest. 1997;57:111–118. - PubMed
-
- Smith RP, Lipworth BJ, Cree IA, et al. C-reactive protein. A clinical marker in community-acquired pneumonia. Chest. 1995;108:1288–1291. - PubMed
-
- Smith RP, Lipworth BJ. C-reactive protein in simple community-acquired pneumonia. Chest. 1995;107:1028–1031. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous