

Increase in methicillin-resistant Staphylococcus aureus acquisition rate and change in pathogen pattern associated with an outbreak of severe acute respiratory syndrome
- PMID: 15356814
- PMCID: PMC7204093
- DOI: 10.1086/422641
Increase in methicillin-resistant Staphylococcus aureus acquisition rate and change in pathogen pattern associated with an outbreak of severe acute respiratory syndrome
Abstract
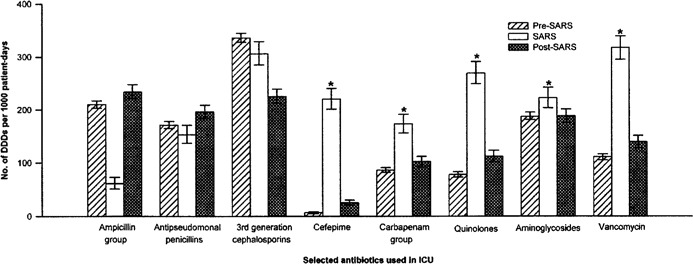
Background: An outbreak of severe acute respiratory syndrome (SARS) occurred in our 22-bed intensive care unit (ICU; Prince of Wales Hospital, Hong Kong, HKSAR, China) from 12 March to 31 May 2003, when only patients with SARS were admitted. This period was characterized by the upgrading of infection control precautions, which included the wearing of gloves and gowns all the time, an extensive use of steroids, and a change in antibiotic prescribing practices. The pattern of endemic pathogenic organisms, the rates of acquisition of methicillin-resistant Staphylococcus aureus (MRSA), and the rates of ventilator-associated pneumonia (VAP) were compared with those of the pre-SARS and post-SARS periods.
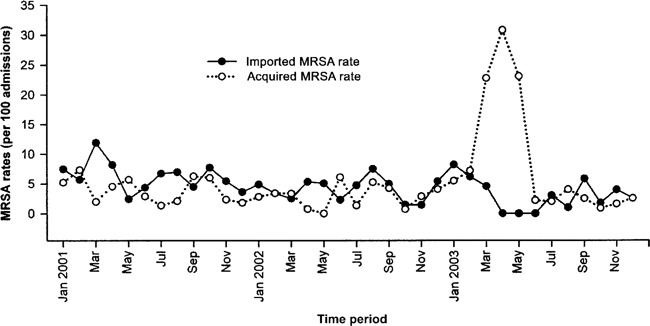
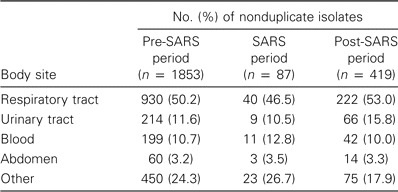
Methods: Data on pathogenic isolates were obtained from the microbiology department (Prince of Wales Hospital). Data on MRSA acquisition and VAP rates were collected prospectively. MRSA screening was performed for all ICU patients. A case of MRSA carriage was defined as an instance in which MRSA was recovered from any site in a patient, and cases were classified as imported or ICU-acquired if the first MRSA isolate was recovered within 72 h of ICU admission or after 72 h in the ICU, respectively.
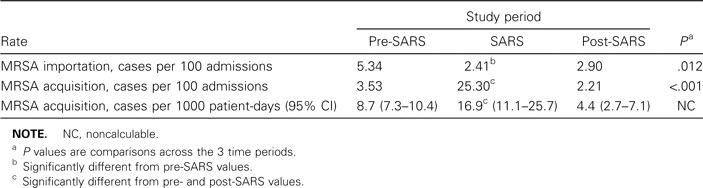
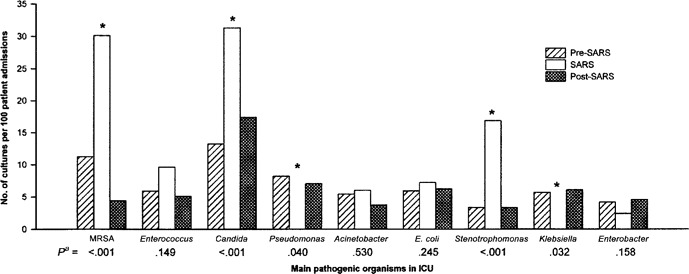
Results: During the SARS period in the ICU, there was an increase in the rate of isolation of MRSA and Stenotrophomonas and Candida species but a disappearance of Pseudomonas and Klebsiella species. The MRSA acquisition rate was also increased: it was 3.53% (3.53 cases per 100 admissions) during the pre-SARS period, 25.30% during the SARS period, and 2.21% during the post-SARS period (P<.001). The VAP rate was high, at 36.5 episodes per 1000 ventilator-days, and 47% of episodes were caused by MRSA.
Conclusions: A SARS outbreak in the ICU led to changes in the pathogen pattern and the MRSA acquisition rate. The data suggest that MRSA cross-transmission may be increased if gloves and gowns are worn all the time.
Figures
Comment in
-
Paradoxical increase in methicillin-resistant Staphylococcus aureus acquisition rates despite barrier precautions and increased hand washing compliance during an outbreak of severe acute respiratory syndrome.Clin Infect Dis. 2005 Feb 15;40(4):632-3. doi: 10.1086/427150. Clin Infect Dis. 2005. PMID: 15712092 Free PMC article. No abstract available.
-
Outbreak of methicillin-resistant Staphylococcus aureus infection associated with an outbreak of severe acute respiratory syndrome.Clin Infect Dis. 2005 Feb 15;40(4):633-4; author reply 634-5. doi: 10.1086/427151. Clin Infect Dis. 2005. PMID: 15712093 Free PMC article. No abstract available.
References
-
- World Health Organization . Summary table of SARS cases by country, 1 November 2002-7 August 2003. 2003. Available at: http://www.who.int/csr/sars/country/2003_08_15/en/. Accessed 20 November 2003.
-
- Centers for Disease Control Prevention Cluster of severe acute respiratory syndrome cases among protected health-care workers—Toronto, Canada, April 2003. MMWR Morb Mortal Wkly Rep. 2003;52:433–6. - PubMed
-
- Lee N, Hui D, Wu A, et al. A major outbreak of severe acute respiratory syndrome in Hong Kong. N Engl J Med. 2003;348:1986–94. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
