

The Munich Barrett follow up study: suspicion of Barrett's oesophagus based on either endoscopy or histology only--what is the clinical significance?
- PMID: 15361485
- PMCID: PMC1774245
- DOI: 10.1136/gut.2003.036822
The Munich Barrett follow up study: suspicion of Barrett's oesophagus based on either endoscopy or histology only--what is the clinical significance?
Abstract
Background: The incidence of distal oesophageal adenocarcinoma is rising, with chronic reflux and Barrett's oesophagus being considered risk factors. Reliable detection of Barrett's oesophagus during upper endoscopy is therefore mandatory but requires both endoscopy and histology for confirmation. Appropriate management of patients with endoscopic suspicion but negative on histology, or vice versa, or of patients with no endoscopic suspicion but with a biopsy diagnosis of intestinal metaplasia at the gastro-oesophageal junction, has not yet been studied prospectively.
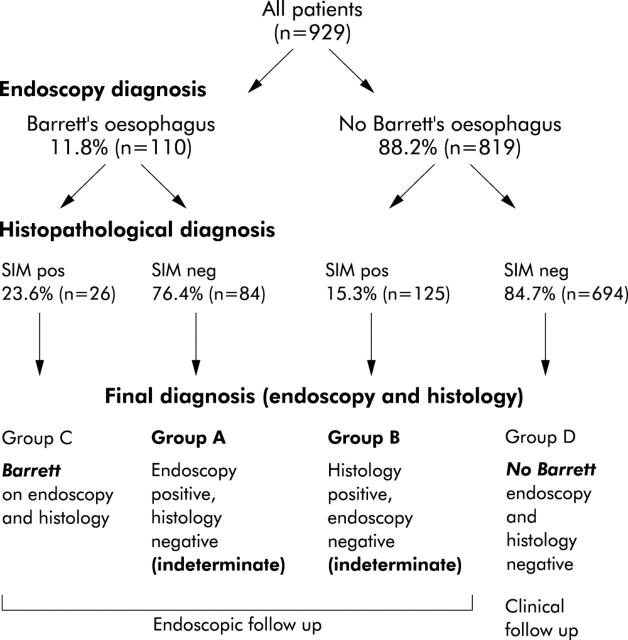
Patients and methods: In a prospective multicentre study, 929 patients (51% male, mean age 50 years) referred for upper gastrointestinal endoscopy were included; 59% had reflux symptoms. The endoscopic aspect of the Z line and any suspicion of Barrett's oesophagus were noted, and biopsies were taken in all patients from the Z line (n = 4), gastric cardia (n = 2), and body and antrum (n = 2 each). Biopsies positive for specialised intestinal metaplasia (SIM) were reviewed by a reference pathologist for a final Barrett's oesophagus diagnosis. All patients with endoscopic and/or histological suspicion of Barrett's oesophagus were invited for a follow up endoscopy; the remaining cases (no endoscopic or histological suspicion of Barrett's oesophagus) were followed clinically.
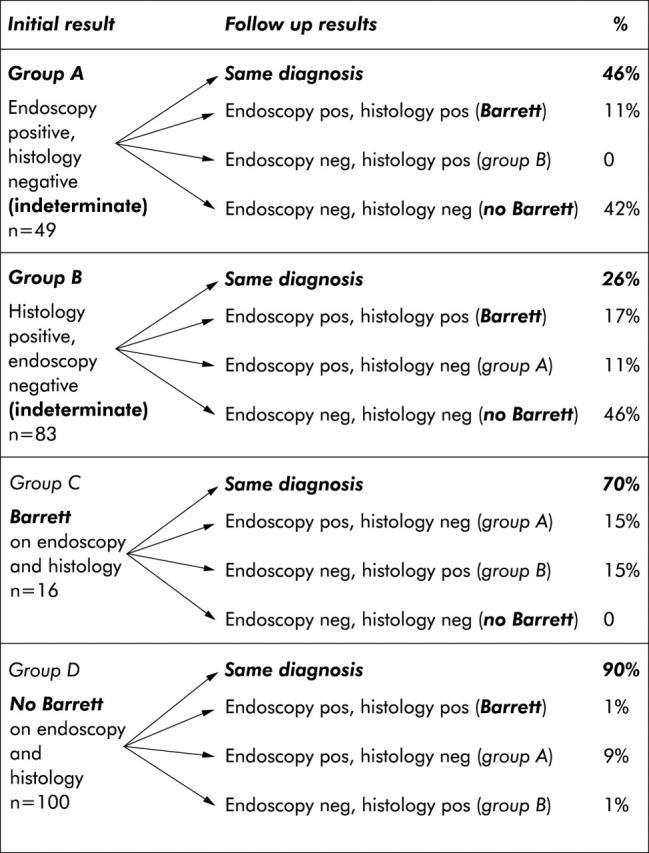
Results: Of 235 patients positive for Barrett's oesophagus on endoscopy and/or histology, 63% agreed to undergo repeat endoscopy (mean follow up period 30.5 months). 46% of patients with an endoscopic Barrett's oesophagus diagnosis but no histological confirmation (group A) showed the same distribution, a further 42% did not have Barrett's oesophagus, and 11% had confirmed Barrett's oesophagus on both endoscopy and biopsy on follow up. In the group with a histological Barrett's oesophagus diagnosis but negative on initial endoscopy (group B), follow up showed the same in 26% whereas 46% had no Barrett's oesophagus, and confirmed Barrett's oesophagus (endoscopy plus histology) was diagnosed in 17%. Of the study population, 16 patients had Barrett's oesophagus on initial endoscopy confirmed by histology which remained constant in 70% at follow up (group C). Of the remaining patients without an initial Barrett's oesophagus diagnosis on either endoscopy or histology (group D) and only clinical follow up (mean follow up period 38 months), one confirmed Barrett's oesophagus case was found among 100 patients re-endoscoped outside of the study protocol. However, no single case of dysplasia or cancer of the distal oesophagus was detected in any patient during the study period.
Conclusions: Even in a specialised gastroenterology setting, reproducibility of presumptive endoscopic or histological diagnoses of Barrett's oesophagus at follow up were poor. Only 10-20% of cases with either endoscopic or histological suspicion of Barrett's oesophagus had established Barrett's oesophagus after 2.5 years of follow up. The risk of dysplasia in this population was very low and hence meticulous follow up may not be required.
Figures
Similar articles
-
[The influence of Barrett's esophagus on the clinical signs and postoperative results of GERD].Zentralbl Chir. 2004 Apr;129(2):99-103. doi: 10.1055/s-2004-816278. Zentralbl Chir. 2004. PMID: 15106039 German.
-
Prospective multivariate analysis of clinical, endoscopic, and histological factors predictive of the development of Barrett's multifocal high-grade dysplasia or adenocarcinoma.Am J Gastroenterol. 1999 Dec;94(12):3413-9. doi: 10.1111/j.1572-0241.1999.01602.x. Am J Gastroenterol. 1999. PMID: 10606296
-
Dysplasia in short-segment Barrett's esophagus: a prospective 3-year follow-up.Am J Gastroenterol. 1997 Nov;92(11):2012-6. Am J Gastroenterol. 1997. PMID: 9362182
-
Barrett's oesophagus: diagnosis and management.Baillieres Best Pract Res Clin Gastroenterol. 2000 Oct;14(5):857-79. doi: 10.1053/bega.2000.0129. Baillieres Best Pract Res Clin Gastroenterol. 2000. PMID: 11003814 Review.
-
Diagnosis and treatment of Barrett's oesophagus. A general survey.Acta Chir Belg. 2001 Mar-Apr;101(2):53-8. Acta Chir Belg. 2001. PMID: 11396051 Review.
Cited by
-
Does Sleeve Gastrectomy Increase the Risk of Barret's Esophagus?Obes Surg. 2021 Jan;31(1):101-110. doi: 10.1007/s11695-020-04875-9. Epub 2020 Jul 29. Obes Surg. 2021. PMID: 32725593
-
Histologic Features Associated With Columnar-lined Esophagus in Distal Esophageal and Gastroesophageal Junction (GEJ) Biopsies From GERD Patients: A Community-based Population Study.Am J Surg Pathol. 2016 Jun;40(6):827-35. doi: 10.1097/PAS.0000000000000623. Am J Surg Pathol. 2016. PMID: 26927889 Free PMC article.
-
Elevated expression of the IGF2 mRNA binding protein 2 (IGF2BP2/IMP2) is linked to short survival and metastasis in esophageal adenocarcinoma.Oncotarget. 2016 Aug 2;7(31):49743-49750. doi: 10.18632/oncotarget.10439. Oncotarget. 2016. PMID: 27391348 Free PMC article.
-
The value of traditional upper endoscopy as a diagnostic test for Barrett's esophagus.Gastrointest Endosc. 2008 Nov;68(5):859-66. doi: 10.1016/j.gie.2008.02.064. Epub 2008 Jun 2. Gastrointest Endosc. 2008. PMID: 18514655 Free PMC article.
-
Histopathology of the endoscopic esophagogastric junction in patients with gastroesophageal reflux disease.Wien Klin Wochenschr. 2008;120(11-12):350-9. doi: 10.1007/s00508-008-0997-2. Wien Klin Wochenschr. 2008. PMID: 18709523
References
-
- Pera M , Cameron AJ, Trastek VF, et al. Increasing incidence of adenocarcinoma of the esophagus and esophagogastric junction. Gastroenterology 1993;104:510–13. - PubMed
-
- Devesa SS, Blot WJ, Fraumeni JF. Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer 1998;83:2049–53. - PubMed
-
- Sampliner RE, and the Practice Parameters Committee of the American College of Gastroenterology. Updated practice guidelines on the diagnosis, surveillance, and therapy of Barrett’s esophagus. Am J Gastroenterol 2002;97:1888–95. - PubMed
-
- Provencale D , Schmitt C, Wong JB. Barrett’s esophagus: a new look at surveillance based on emerging estimates of cancer risk. Am J Gastroenterol 1999;94:2043–53. - PubMed
-
- Spechler SJ, Zeroogian JM, Antonioli DA, et al. Prevalence of metaplasia at the gastro-oesophageal junction. Lancet 1994;344:1533–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical