

CD4+ T cell depletion during all stages of HIV disease occurs predominantly in the gastrointestinal tract
- PMID: 15365096
- PMCID: PMC2211962
- DOI: 10.1084/jem.20040874
CD4+ T cell depletion during all stages of HIV disease occurs predominantly in the gastrointestinal tract
Abstract
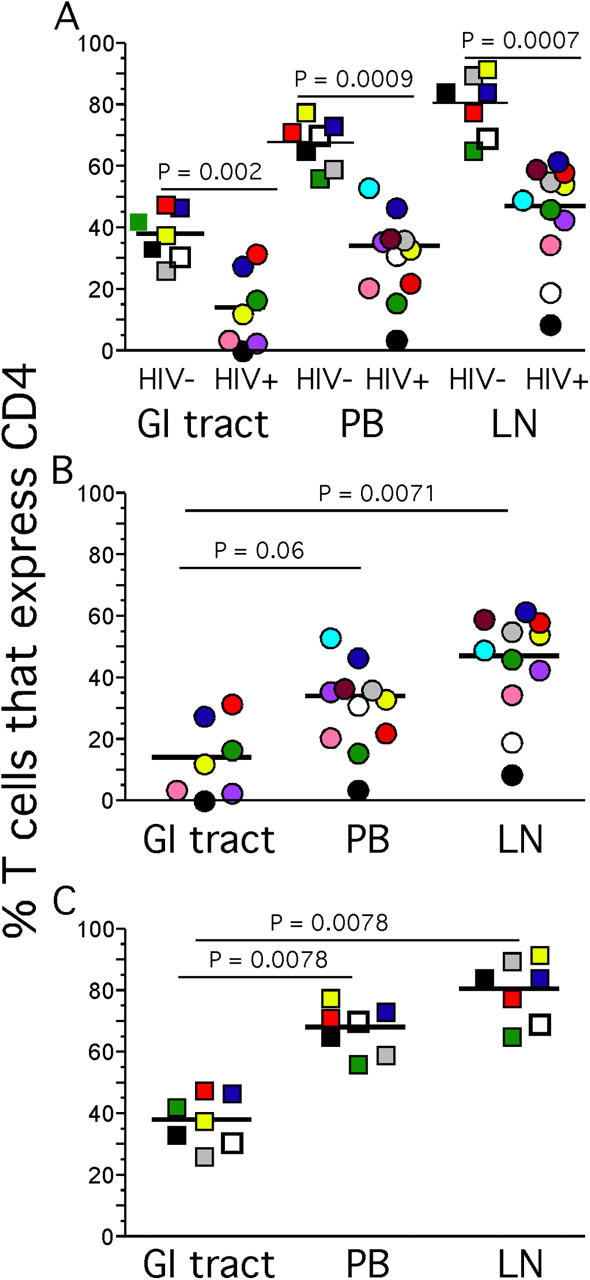
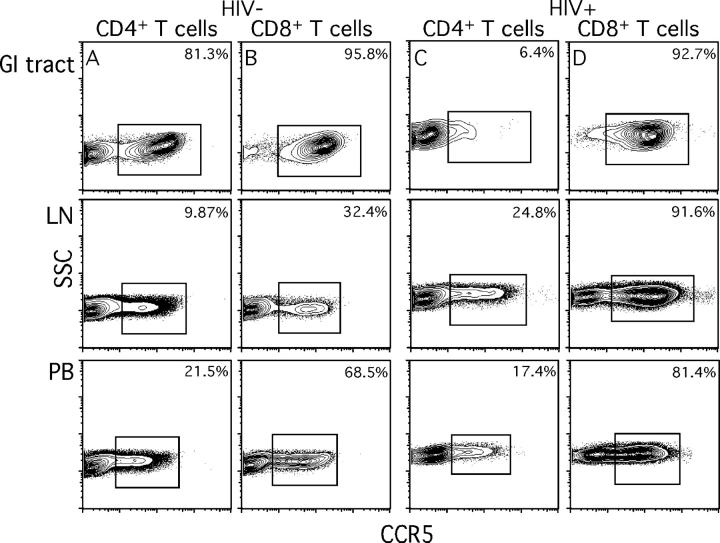
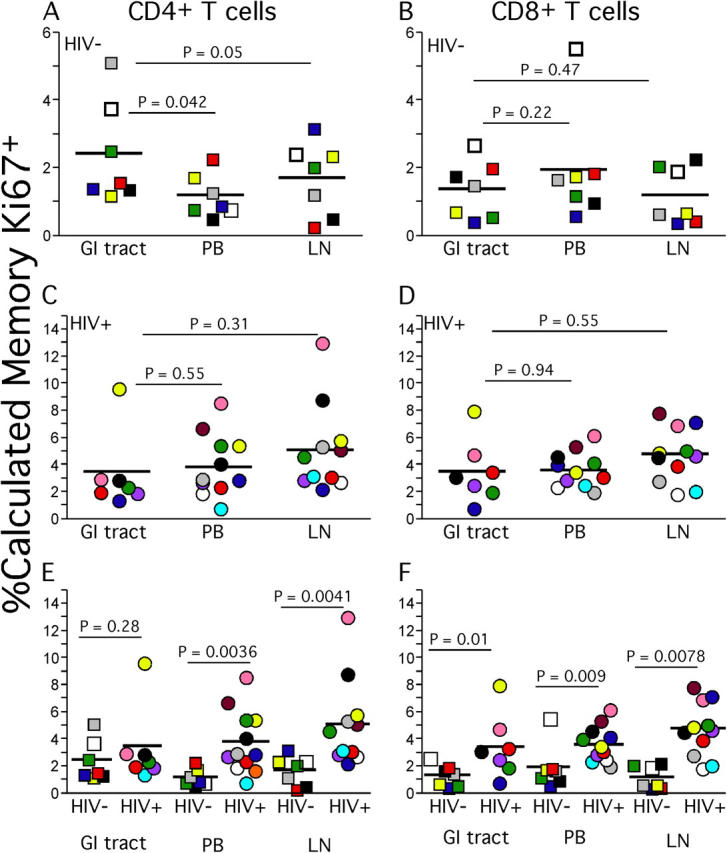
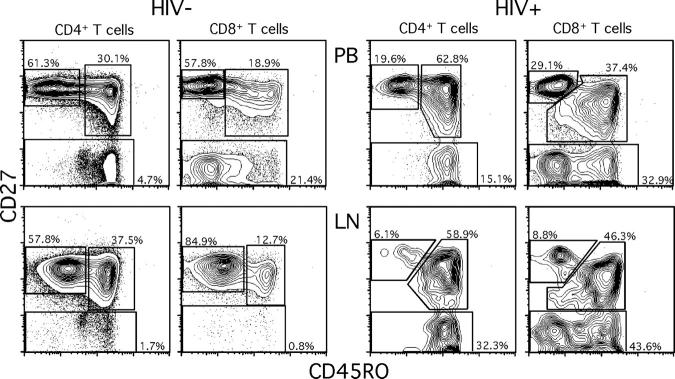
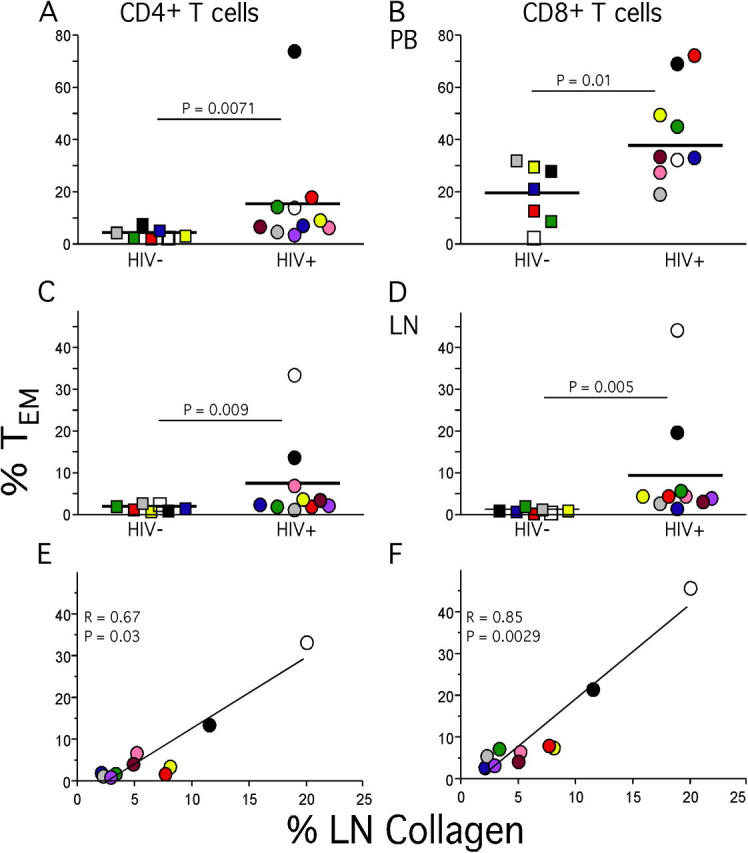
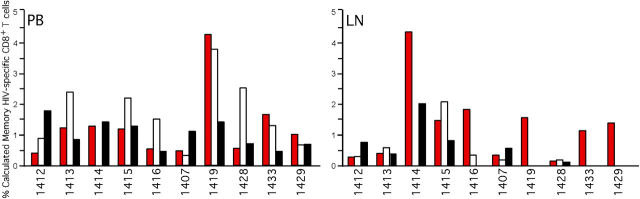
The mechanisms underlying CD4(+) T cell depletion in human immunodeficiency virus (HIV) infection are not well understood. Comparative studies of lymphoid tissues, where the vast majority of T cells reside, and peripheral blood can potentially illuminate the pathogenesis of HIV-associated disease. Here, we studied the effect of HIV infection on the activation and depletion of defined subsets of CD4(+) and CD8(+) T cells in the blood, gastrointestinal (GI) tract, and lymph node (LN). We also measured HIV-specific T cell frequencies in LNs and blood, and LN collagen deposition to define architectural changes associated with chronic inflammation. The major findings to emerge are the following: the GI tract has the most substantial CD4(+) T cell depletion at all stages of HIV disease; this depletion occurs preferentially within CCR5(+) CD4(+) T cells; HIV-associated immune activation results in abnormal accumulation of effector-type T cells within LNs; HIV-specific T cells in LNs do not account for all effector T cells; and T cell activation in LNs is associated with abnormal collagen deposition. Taken together, these findings define the nature and extent of CD4(+) T cell depletion in lymphoid tissue and point to mechanisms of profound depletion of specific T cell subsets related to elimination of CCR5(+) CD4(+) T cell targets and disruption of T cell homeostasis that accompanies chronic immune activation.
Figures

References
-
- Dybul, M., A.S. Fauci, J.G. Bartlett, J.E. Kaplan, and A.K. Pau. 2002. Guidelines for using antiretroviral agents among HIV-infected adults and adolescents. Recommendations of the Panel on Clinical Practices for Treatment of HIV. MMWR Recomm. Rep. 51:1–55. - PubMed
-
- Mowat, A., and J. Viney. 1997. The anatomical basis of intestinal immunity. Immunol. Rev. 156:145–166. - PubMed
-
- Anton, P.A., J. Elliott, M.A. Poles, I.M. McGowan, J. Matud, L.E. Hultin, K. Grovit-Ferbas, C.R. Mackay, I.S.Y. Chen, and J.V. Giorgi. 2000. Enhanced levels of functional HIV-1 co-receptors on human mucosal T cells demonstrated using intestinal biopsy tissue. AIDS. 14:1761–1765. - PubMed
-
- Agace, W.W., A.I. Roberts, L. Wu, C. Greineder, E.C. Ebert, and C.M. Parker. 2000. Human intestinal lamina propria and intraepithelial lymphocytes express receptors specific for chemokines induced by inflammation. Eur. J. Immunol. 30:819–826. - PubMed
-
- Veazey, R.S., M. DeMaria, L.V. Chalifoux, D.E. Shvetz, D.R. Pauley, H.L. Knight, M. Rosenzweig, R.P. Johnson, R.C. Desrosiers, and A.A. Lackner. 1998. Gastrointestinal tract as a major site of CD4+ T cell depletion and viral replication in SIV infection. Science. 280:427–431. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
