

Death and renal transplantation among Aboriginal people undergoing dialysis
- PMID: 15367459
- PMCID: PMC516192
- DOI: 10.1503/cmaj.1031859
Death and renal transplantation among Aboriginal people undergoing dialysis
Abstract
Background: Despite the increase in the number of Aboriginal people with end-stage renal disease around the world, little is known about their health outcomes when undergoing renal replacement therapy. We evaluated differences in survival and rate of renal transplantation among Aboriginal and white patients after initiation of dialysis.
Methods: Adult patients who were Aboriginal or white and who commenced dialysis in Alberta, Saskatchewan or Manitoba between Jan. 1, 1990, and Dec. 31, 2000, were recruited for the study and were followed until death, transplantation, loss to follow-up or the end of the study (Dec. 31, 2001). We used Cox proportional hazards models to examine the effect of race on patient survival and likelihood of transplant, with adjustment for potential confounders.
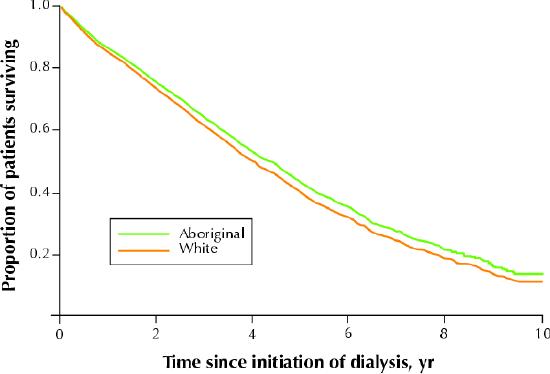
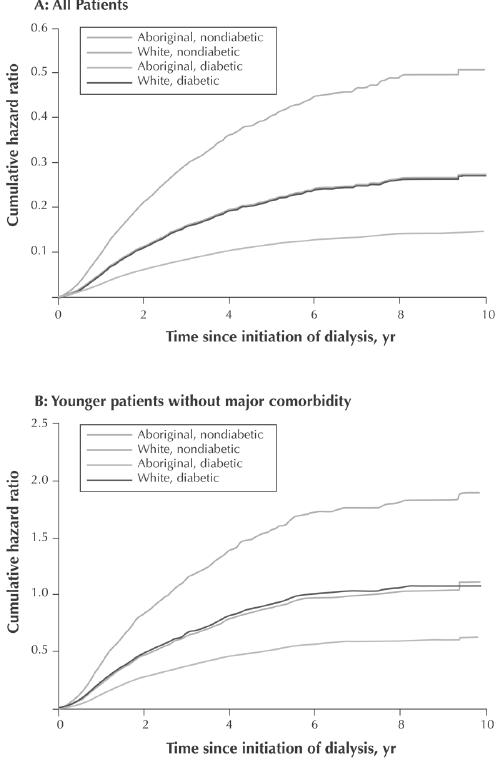
Results: Of the 4333 adults who commenced dialysis during the study period, 15.8% were Aboriginal and 72.4% were white. Unadjusted rates of death per 1000 patient-years during the study period were 158 (95% confidence interval [CI] 144-176) for Aboriginal patients and 146 (95% CI 139-153) for white patients. When follow-up was censored at the time of transplantation, the age-adjusted risk of death after initiation of dialysis was significantly higher among Aboriginal patients than among white patients (hazard ratio [HR] 1.15, 95% CI 1.02-1.30). The greater risk of death associated with Aboriginal race was no longer observed after adjustment for diabetes mellitus and other comorbid conditions (adjusted HR 0.89, 95% CI 0.77-1.02) and did not appear to be associated with socioeconomic status. During the study period, unadjusted transplantation rates per 1000 patient-years were 62 (95% CI 52-75) for Aboriginal patients and 133 (95% CI 125-142) for white patients. Aboriginal patients were significantly less likely to receive a renal transplant after commencing dialysis, even after adjustment for potential confounders (HR 0.43, 95% CI 0.35-0.53). In an additional analysis that included follow-up after transplantation for those who received renal allografts, the age-adjusted risk of death associated with Aboriginal race (HR 1.36, 95% CI 1.21-1.52) was higher than when follow-up after transplantation was not considered, perhaps because of the lower rate of transplantation among Aboriginals.
Interpretation: Survival among dialysis patients was similar for Aboriginal and white patients after adjustment for comorbidity. However, despite universal access to health care, Aboriginal people had a significantly lower rate of renal transplantation, which might have adversely affected their survival when receiving renal replacement therapy.
Figures
Comment in
-
Health outcomes in Aboriginal populations.CMAJ. 2004 Sep 14;171(6):597-8. doi: 10.1503/cmaj.1041059. CMAJ. 2004. PMID: 15367462 Free PMC article. No abstract available.
-
The ethics of research involving Canada's Aboriginal populations.CMAJ. 2005 Apr 12;172(8):977; author reply 977-9. doi: 10.1503/cmaj.1041676. CMAJ. 2005. PMID: 15824389 Free PMC article. No abstract available.
References
-
- Burrows NR, Geiss LS, Engelgau MM, Acton KJ. Prevalence of diabetes among Native Americans and Alaska Natives, 1990-1997: an increasing burden. Diabetes Care 2000;23(12):1786-90. - PubMed
-
- Fagot-Campagna A, Pettitt DJ, Engelgau MM, Burrows NR, Geiss LS, Valdez R, et al. Type 2 diabetes among North American children and adolescents: an epidemiologic review and a public health perspective. J Pediatr 2000; 136 (5):664-72. - PubMed
-
- Daniel M, Rowley KG, McDermott R, Mylvaganam A, O'Dea K. Diabetes incidence in an Australian aboriginal population. An 8-year follow-up study. Diabetes Care 1999;22(12):1993-8. - PubMed
-
- McDonald SP, Russ GR. Burden of end-stage renal disease among indigenous peoples in Australia and New Zealand. Kidney Int Suppl 2003;(83):S123-7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials