

Review
doi: 10.1172/JCI22991.
Trophoblast differentiation during embryo implantation and formation of the maternal-fetal interface
Affiliations
- PMID: 15372095
- PMCID: PMC516273
- DOI: 10.1172/JCI22991
Item in Clipboard
Review
Trophoblast differentiation during embryo implantation and formation of the maternal-fetal interface
J Clin Invest.
2004 Sep.
Abstract
Trophoblasts, the specialized cells of the placenta, play a major role in implantation and formation of the maternal-fetal interface. Through an unusual differentiation process examined in this review, these fetal cells acquire properties of leukocytes and endothelial cells that enable many of their specialized functions. In recent years a great deal has been learned about the regulatory mechanisms, from transcriptional networks to oxygen tension, which control trophoblast differentiation. The challenge is to turn this information into clinically useful tests for monitoring placental function and, hence, pregnancy outcome.
Figures
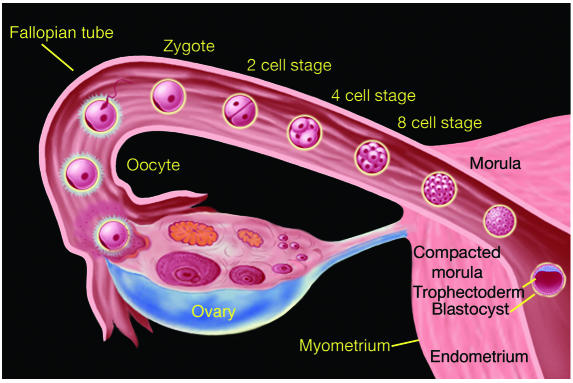
The early stages of human development from fertilization to blastocyst formation. Fertilization occurs in the fallopian tube within 24 to 48 hours of ovulation. The initial stages of development, from fertilized ovum (zygote) to a solid mass of cells (morula), occur as the embryo passes through the fallopian tube encased within a nonadhesive protective shell (the zona pellucida). The morula enters the uterine cavity approximately two to three days after fertilization. The appearance of a fluid-filled inner cavity marks the transition from morula to blastocyst and is accompanied by cellular differentiation: the surface cells become the trophoblast (and give rise to extraembryonic structures, including the placenta) and the inner cell mass gives rise to the embryo. Within 72 hours of entering the uterine cavity, the embryo hatches from the zona, thereby exposing its outer covering of trophectoderm. Figure kindly provided by S.S. Gambhir and J. Strommer, Stanford University (Stanford, California, USA).

Implantation in humans involves a number of the molecular mechanisms that mediate leukocyte emigration from the blood to sites of inflammation or injury. The diagram was made from a combination of images: MECA-79 antibody staining of uterine tissue sections and L-selectin antibody staining of cultured embryos. Recently acquired evidence suggests that an implantation-competent human blastocyst expresses L-selectin on its surface (green). This receptor interacts with specialized carbohydrate ligands, including sulfated species, recognized by the MECA-79 antibody, which stains the uterine luminal and glandular epithelium. The specialized nature of these interactions translates into an unusual form of cell adhesion: rolling and tethering. In the uterus, MECA-79 immunoreactivity peaks during the window of receptivity. This finding suggests that apposition, the first step in implantation, includes L-selectin_mediated tethering of the blastocyst to the upper portion of the posterior wall of the uterine fundus.

Oxygen tension plays an important role in guiding the differentiation process that leads to cytotrophoblast invasion of the uterus. (A) The early stages of placental development take place in a relatively hypoxic environment that favors cytotrophoblast proliferation rather than differentiation along the invasive pathway. Accordingly, this cell population (light green cells) rapidly increases in number as compared with the embryonic lineages. (B) As development continues, cytotrophoblasts (dark green cells) invade the uterine wall and plug the maternal vessels, a process that helps maintain a state of physiological hypoxia. As indicated by the blunt arrows, cytotrophoblasts migrate farther up arteries than veins. (C) By 10 to 12 weeks of human pregnancy, blood flow to the intervillous space begins. As the endovascular component of cytotrophoblast invasion progresses, the cells migrate along the lumina of spiral arterioles, replacing the maternal endothelial lining. Cytotrophoblasts are also found in the smooth muscle walls of these vessels. In normal pregnancy the process whereby placental cells remodel uterine arterioles involves the decidual and inner third of the myometrial portions of these vessels. As a result, the diameter of the arterioles expands to accommodate the dramatic increase in blood flow that is needed to support rapid fetal growth later in pregnancy. It is likely that failed endovascular invasion leads, in some cases, to abortion, whereas an inability to invade to the appropriate depth is associated with preeclampsia and a subset of pregnancies in which the growth of the fetus is restricted.

Illustration of two in vitro models for studying human cytotrophoblast invasion. (A) When human cytotrophoblasts (light green cells encircled in red) are isolated from early-gestation placentas and plated on an extracellular matrix (ECM) substrate (Matrigel), they differentiate along the pathway that leads to uterine invasion. By 12 hours in culture these cells form aggregates that resemble cell columns of anchoring villi, and by 48 hours they switch on expression of a repertoire of stage-specific antigens that are expressed in cytotrophoblasts within the uterine wall in situ (dark green cells). These molecules facilitate uterine invasion, vascular mimicry, and evasion of the maternal immune response. (B) When anchoring villi are dissected from the surfaces of early-gestation human placentas (blue box) and plated on an ECM substrate, cytotrophoblasts in cell columns continue to differentiate. By 48 hours many cytotrophoblasts have left the columns and invaded the substrate (green box). During this process they execute the same phenotypic switch that isolated cells carry out.

In severe preeclampsia as compared to normal pregnancy, cytotrophoblast invasion is shallow and the cells fail to switch on the expression of stage-specific antigens that are normally upregulated as they penetrate the uterine wall and blood vessels (BVs). (A and C) Cytokeratin (CK) staining of tissue sections of the maternal-fetal interface allows visualization of cytotrophoblasts that invade the uterine wall. (B) In normal pregnancy, the subpopulation of human cytotrophoblasts that carries out endovascular invasion upregulates expression of the neural cell adhesion molecule (NCAM). (D) In cases of severe preeclampsia (SPE), NCAM immunoreactivity is either absent or very weak (indicated by the arrows). AV, anchoring villus; COL, cell column of anchoring villus.
References
-
- Wu L, et al. Extra-embryonic function of Rb is essential for embryonic development and viability. Nature. 2003;421:942–947. - PubMed
-
- Sibai BM, et al. Risk factors associated with preeclampsia in healthy nulliparous women. The Calcium for Preeclampsia Prevention (CPEP) Study Group. Am. J. Obstet. Gynecol. 1997;177:1003–1010. - PubMed
-
- Goldenberg RL, Hauth JC, Andrews WW. Intrauterine infection and preterm delivery. N. Engl. J. Med. 2000;342:1500–1507. - PubMed
-
- Kunath T, Strumpf D, Rossant J. Early trophoblast determination and stem cell maintenance in the mouse-a review. Placenta. 2004;25(Suppl.):S32–S38. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
