

Intraocular lymphoma: update on diagnosis and management
- PMID: 15377987
- PMCID: PMC1971130
- DOI: 10.1177/107327480401100502
Intraocular lymphoma: update on diagnosis and management
Abstract
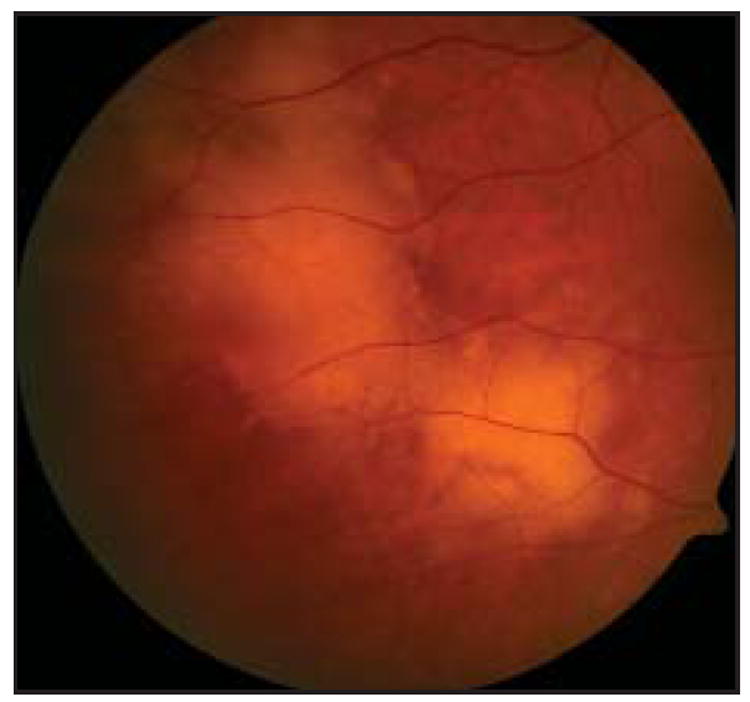
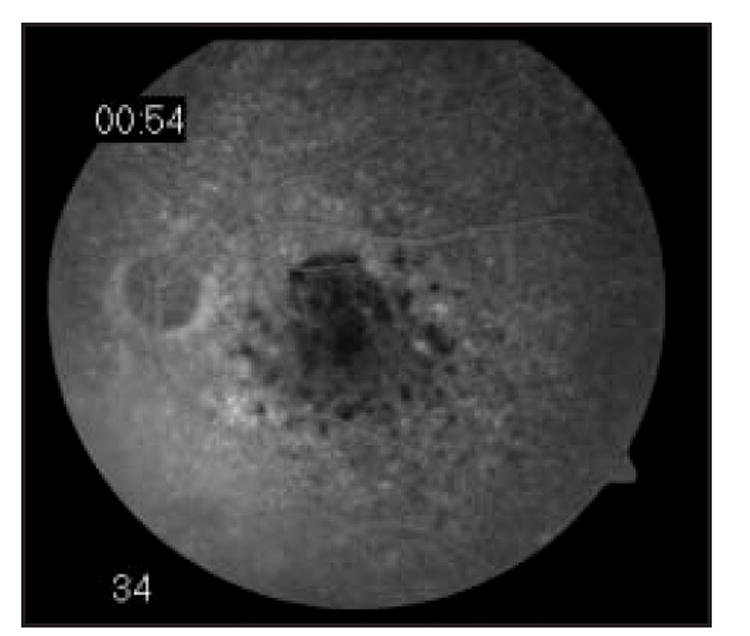
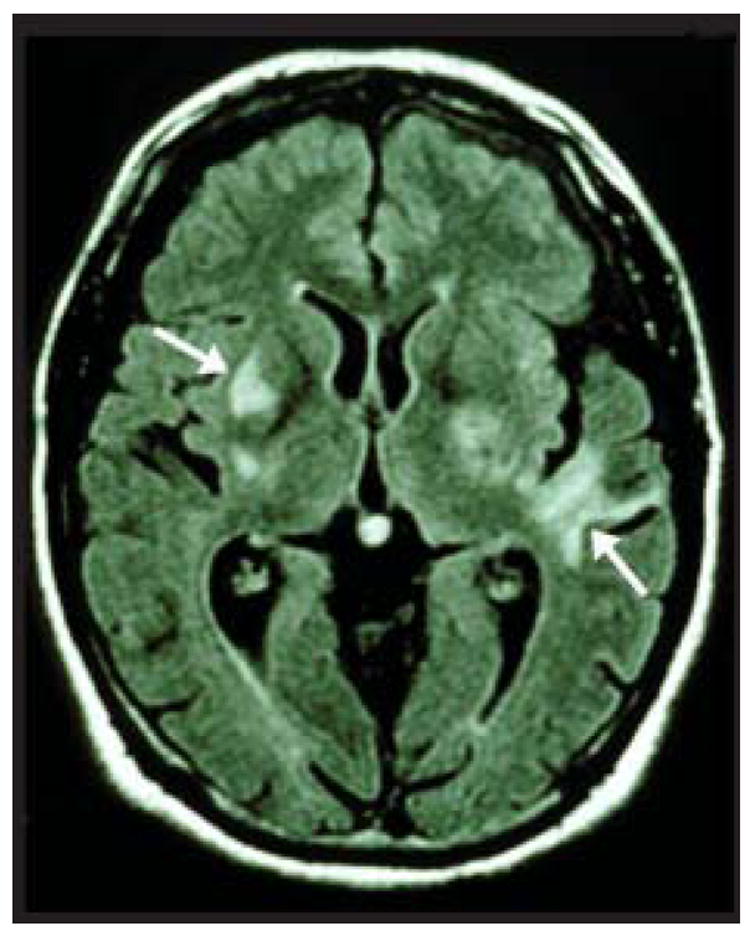
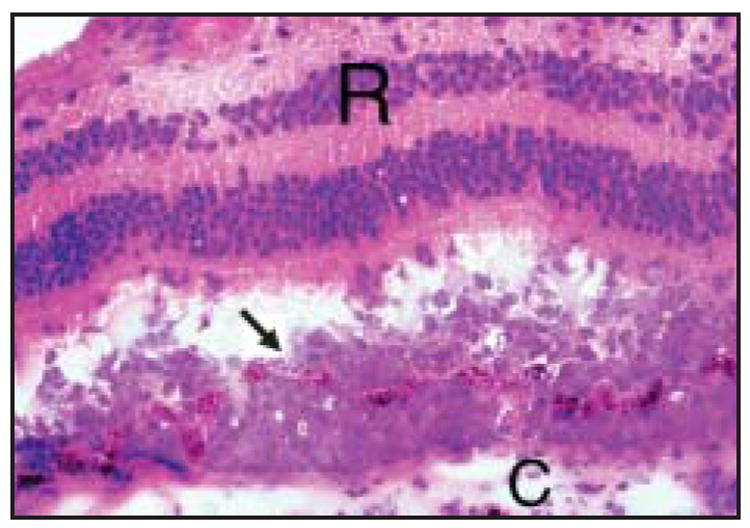
Background: Primary intraocular lymphoma (PIOL) is a subset of primary central nervous system lymphoma (PCNSL) in which lymphoma cells initially invade the retina, vitreous, or optic nerve head, with or without concomitant CNS involvement. The incidence of this previously rare condition has increased dramatically. Given its nonspecific presentation and aggressive course, PIOL provides a diagnostic and therapeutic challenge.
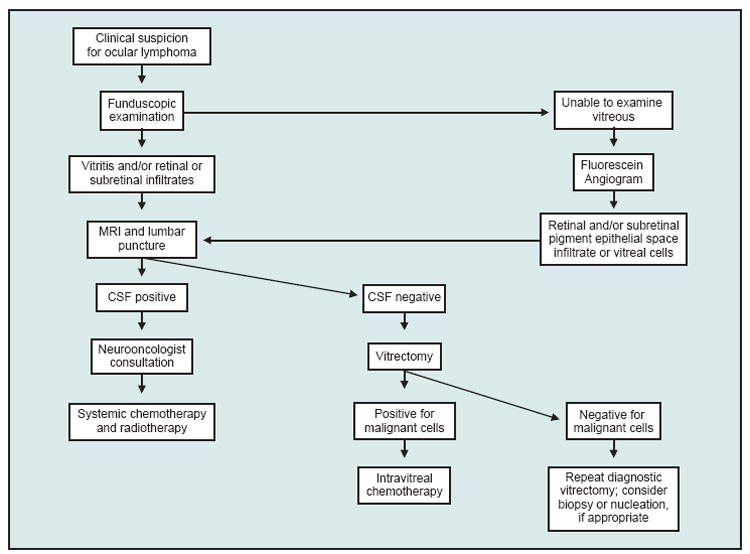
Methods: We review the current strategies for diagnosis and treatment of PIOL and present our own experience with PIOL.
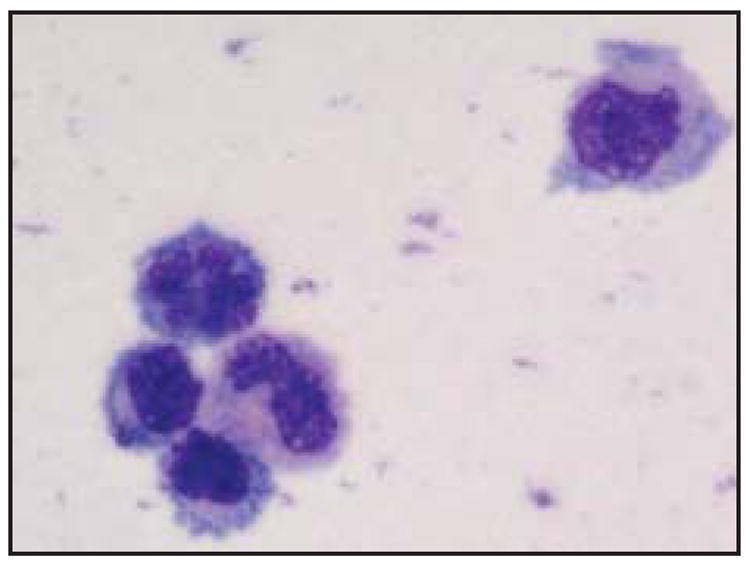
Results: Recent developments in the diagnosis of PIOL include immunohistochemistry, flow cytometry, cytokine evaluation, and molecular analysis. However, definitive diagnosis still requires harvesting of tissue for histopathology. Optimal treatment for PIOL remains unclear. Initial therapeutic regimens should include methotrexate-based chemotherapy and radiotherapy to the brain and eye. In addition, promising results have been seen with intravitreal methotrexate and autologous stem cell transplantation for recurrent and refractory disease.
Conclusions: Efforts to further determine the immunophenotype and molecular characteristics of PIOL will continue to assist in the diagnosis of PIOL. Future studies are required to determine the role of radiotherapy and optimal local and systemic chemotherapeutic regimens.
Figures
References
-
- Hochberg FH, Miller DC. Primary central nervous system lymphoma. J Neurosurg. 1988;68:835–853. - PubMed
-
- Chan CC, Buggage RR, Nussenblatt RB. Intraocular Lymphoma. Curr Opin Ophthalmol. 2002;13:411–418. - PubMed
-
- Hormigo A, DeAngelis LM. Primary ocular lymphoma: clinical features, diagnosis, and treatment. Clin Lymphoma. 2003;4:22–29. - PubMed
-
- Appen RE. Posterior uveitis and primary cerebral reticulum cell sarcoma. Arch Ophthalmol. 1975;93:123–124. - PubMed
-
- Volcker HE, Naumann GO. “Primary” reticulum cell sarcoma of the retina. Dev Ophthalmol. 1981;2:114–120. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
