

Extracorporeal life support for severe acute respiratory distress syndrome in adults
- PMID: 15383787
- PMCID: PMC1356461
- DOI: 10.1097/01.sla.0000141159.90676.2d
Extracorporeal life support for severe acute respiratory distress syndrome in adults
Abstract
Objective: Severe acute respiratory distress syndrome (ARDS) is associated with a high level of mortality. Extracorporeal life support (ECLS) during severe ARDS maintains oxygen and carbon dioxide gas exchange while providing an optimal environment for recovery of pulmonary function. Since 1989, we have used a protocol-driven algorithm for treatment of severe ARDS, which includes the use of ECLS when standard therapy fails. The objective of this study was to evaluate our experience with ECLS in adult patients with severe ARDS with respect to mortality and morbidity.
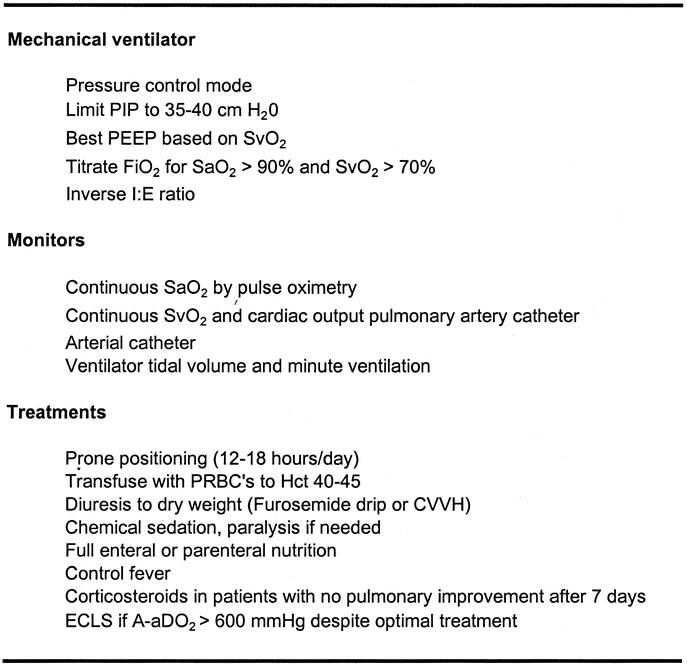
Methods: We reviewed our complete experience with ELCS in adults from January 1, 1989, through December 31, 2003. Severe ARDS was defined as acute onset pulmonary failure, with bilateral infiltrates on chest x-ray, and PaO2/fraction of inspired oxygen (FiO2) ratio < or =100 or A-aDO2 >600 mm Hg despite maximal ventilator settings. The indication for ECLS was acute severe ARDS unresponsive to optimal conventional treatment. The technique of ECLS included veno-venous or veno-arterial vascular access, lung "rest" at low FiO2 and inspiratory pressure, minimal anticoagulation, and optimization of systemic oxygen delivery.
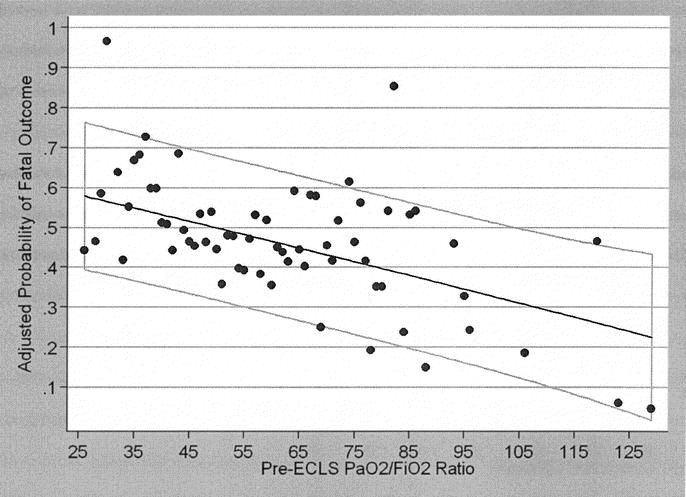
Results: During the study period, ECLS was used for 405 adult patients age 17 or older. Of these 405 patients, 255 were placed on ECLS for severe ARDS refractory to all other treatment. Sixty-seven percent were weaned off ECLS, and 52% survived to hospital discharge. Multivariate logistic regression analysis identified the following pre-ELCS variables as significant independent predictors of survival: (1) age (P = 0.01); (2) gender (P = 0.048); (3) pH < or =7.10 (P = 0.01); (4) PaO2/FiO2 ratio (P = 0.03); and (5) days of mechanical ventilation (P < 0.001). None of the patients who survived required permanent mechanical ventilation or supplemental oxygen therapy.
Conclusion: Extracorporeal life support for severe ARDS in adults is a successful therapeutic option in those patients who do not respond to conventional mechanical ventilator strategies.
Figures
References
-
- Hemmila MR, Hirschl RB. Advances in ventilatory support of the pediatric surgical patient. Curr Opin Pediatr. 1999;11:241–248. - PubMed
-
- Vasilyev S, Schaap RN, Mortensen JD. Hospital survival rates of patients with acute respiratory failure in modern respiratory intensive care units: an international, multicenter, prospective survey. Chest. 1995;107:1083–1088. - PubMed
-
- Weg JG, Anzueto A, Balk RA, et al. The relation of pneumothorax and other air leaks to mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;338:341–346. - PubMed
-
- Luhr OR, Antonsen K, Karlsson M, et al. Incidence and mortality after acute respiratory failure and acute respiratory distress syndrome in Sweden, Denmark, and Iceland. Am J Respir Crit Care Med. 1999;159:1849–1861. - PubMed
-
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
