

Transplantation for type I diabetes: comparison of vascularized whole-organ pancreas with isolated pancreatic islets
- PMID: 15383791
- PMCID: PMC1356465
- DOI: 10.1097/01.sla.0000140754.26575.2a
Transplantation for type I diabetes: comparison of vascularized whole-organ pancreas with isolated pancreatic islets
Abstract
Objective: We sought to compare the efficacy, risks, and costs of whole-organ pancreas transplantation (WOP) with the costs of isolated islet transplantation (IIT) in the treatment of patients with type I diabetes mellitus.
Summary background data: A striking improvement has taken place in the results of IIT with regard to attaining normoglycemia and insulin independence of type I diabetic recipients. Theoretically, this minimally invasive therapy should replace WOP because its risks and expense should be less. To date, however, no systematic comparisons of these 2 options have been reported.
Methods: We conducted a retrospective analysis of a consecutive series of WOP and IIT performed at the University of Pennsylvania between September 2001 and February 2004. We compared a variety of parameters, including patient and graft survival, degree and duration of glucose homeostasis, procedural and immunosuppressive complications, and resources utilization.
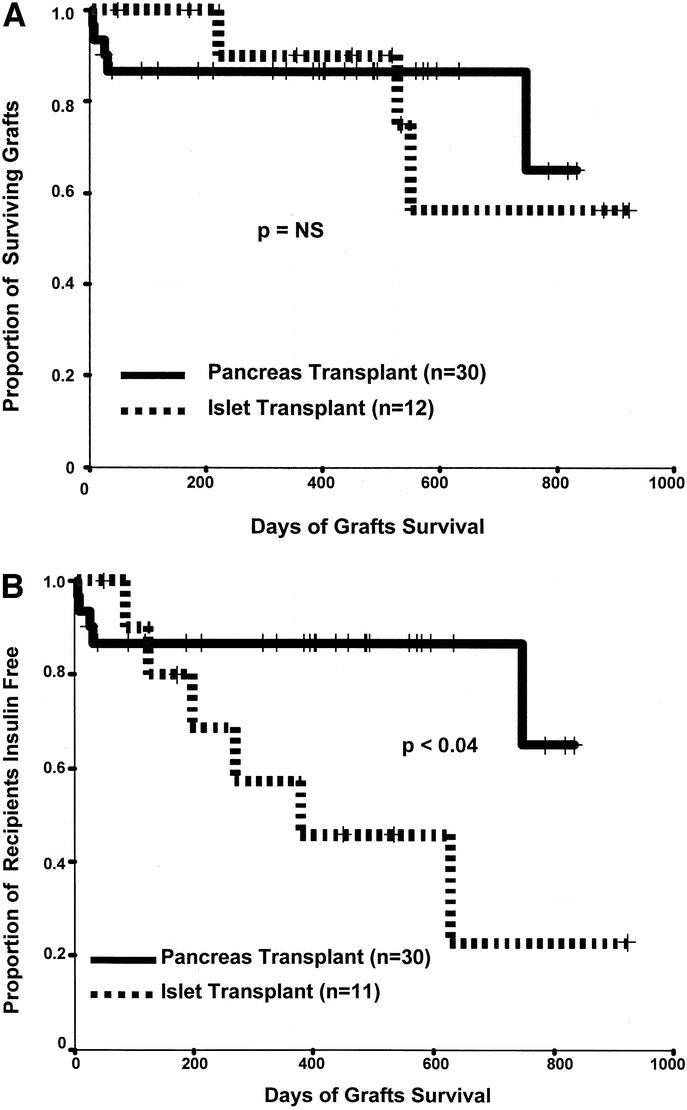
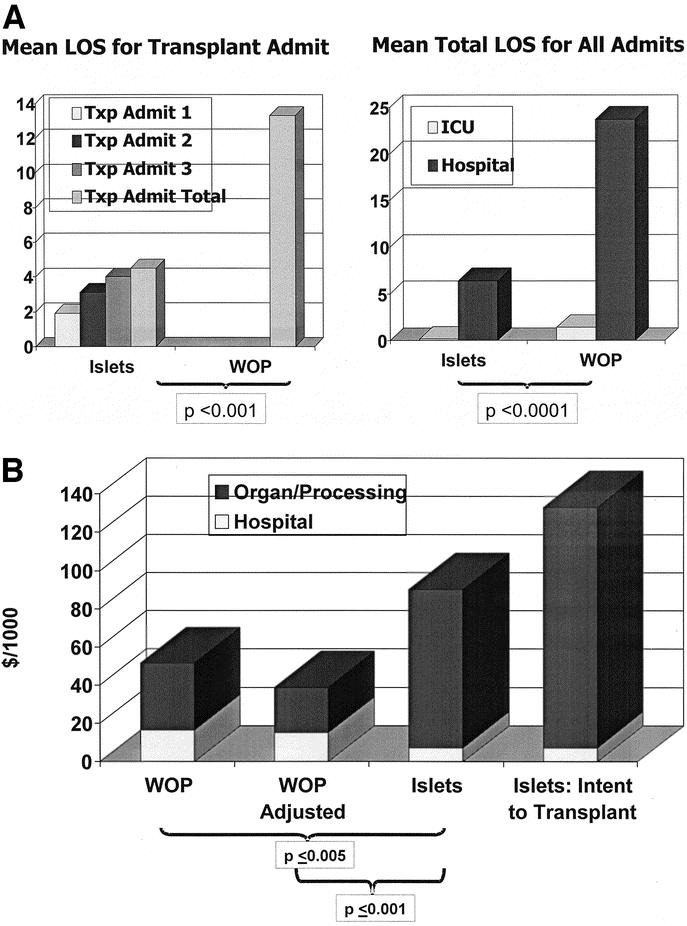
Results: Both WOP and IIT proved highly successful at establishing insulin independence in type I diabetic patients. Whole-organ pancreas recipients experienced longer lengths of stay, more readmissions, and more complications, but they exhibited a more durable state of normoglycemia with greater insulin reserves. Achieving insulin independence by IIT proved surprisingly more expensive, despite shorter initial hospital and readmission stays.
Conclusion: Despite recent improvement in the success of IIT, WOP provides a more reliable and durable restoration of normoglycemia. Although IIT was associated with less procedure-related morbidity and shorter hospital stays, we unexpectedly found IIT to be more costly than WOP. This was largely due to IIT requiring islets from multiple donors to gain insulin independence. Because donor pancreata that are unsuitable for WOP can often be used successfully for IIT, we suggest that as IIT evolves, it should continue to be evaluated as a complementary alternative to rather than as a replacement for the better-established method of WOP.
Figures
References
-
- Kelly W, Lillehei R, Merkel F, et al. Allotranspllantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery. 1967;61:827–837. - PubMed
-
- Ramsay RC, Goetz FC, Sutherland DER, et al. Progression of diabetic retinopathy after pancreas transplantation for insulin-dependent diabetes mellitus. N Engl J Med. 1988;318:208–214. - PubMed
-
- Bilous RW, Mauer SM, Sutherland DER, et al. The effects of pancreas transplantation on the glomerular structure of renal allografts in patients with insulin-dependent diabetes. N Engl J Med. 1989;321:80–85. - PubMed
-
- Fioretto P, Steffes MW, Sutherland DER, et al. Reversal of lesions of diabetic nephropathy after pancreas transplantation. N Engl J Med. 1998;339:69–75. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
