

Improving perioperative outcome expands the role of hepatectomy in management of benign and malignant hepatobiliary diseases: analysis of 1222 consecutive patients from a prospective database
- PMID: 15383797
- PMCID: PMC1356471
- DOI: 10.1097/01.sla.0000141195.66155.0c
Improving perioperative outcome expands the role of hepatectomy in management of benign and malignant hepatobiliary diseases: analysis of 1222 consecutive patients from a prospective database
Abstract
Objective: To assess the trends in perioperative outcome of hepatectomy for hepatobiliary diseases.
Methods: Data of 1222 consecutive patients who underwent hepatectomy for hepatobiliary diseases from July 1989 to June 2003 in a tertiary institution were collected prospectively. Perioperative outcome of patients in the first (group I) and second (group II) halves of this period was compared. Factors associated with morbidity and mortality were analyzed.
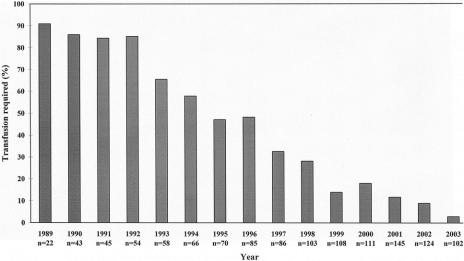
Results: Diagnoses included hepatocellular carcinoma (n = 734), other liver cancers (n = 257), extrahepatic biliary malignancies (n = 43), hepatolithiasis (n = 101), benign liver tumors (n = 61), and other diseases (n = 26). The majority of patients (61.8%) underwent major hepatectomy of > or = 3 segments. The overall hospital mortality and morbidity were 4.9% and 32.4%, respectively. The number of hepatectomies increased from 402 in group I to 820 in group II, partly as a result of more liberal patient selection. Group II had more elderly patients (P = 0.006), more patients with comorbid illnesses (P = 0.001), and significantly worse liver function. Nonetheless, group II had lower blood loss (median 750 versus 1450 mL, P < 0.001), perioperative transfusion (17.3% versus 67.7%, P < 0.001), morbidity (30.0% versus 37.3%, P = 0.012), and hospital mortality (3.7% versus 7.5%, P = 0.004). On multivariate analysis, hypoalbuminemia, thrombocytopenia, elevated serum creatinine, major hepatic resection, and transfusion were the significant predictors of hospital mortality, whereas concomitant extrahepatic procedure, thrombocytopenia, and transfusion were the predictors of morbidity.
Conclusions: Perioperative outcome has improved despite extending the indication of hepatectomy to more high-risk patients. The role of hepatectomy in the management of hepatobiliary diseases can be expanded. Reduced perioperative transfusion is the main contributory factor for improved outcome.
Figures
References
-
- Fortner JG, Blumgart LH. A historic perspective of liver surgery for tumors at the end of the millennium. J Am Coll Surg. 2001;193:210–222. - PubMed
-
- Belghiti J, Hiramatsu K, Benoist S, et al. Seven hundred forty-seven hepatectomies in the 1990s: an update to evaluate the actual risk of liver resection. J Am Coll Surg. 2000;191:38–46. - PubMed
-
- Imamura H, Seyama Y, Kokudo N, et al. One thousand fifty-six hepatectomies without mortality in 8 years. Arch Surg. 2003;138:1198–1206. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
