

A prospective, symptom related, outcomes analysis of 1022 palliative procedures for advanced cancer
- PMID: 15383799
- PMCID: PMC1356473
- DOI: 10.1097/01.sla.0000141707.09312.dd
A prospective, symptom related, outcomes analysis of 1022 palliative procedures for advanced cancer
Abstract
Objective: To prospectively evaluate surgical procedures performed with palliative intent.
Summary background data: There is a paucity of outcomes data necessary to allow sound surgical decision-making and informed consent for palliative procedures.
Methods: Procedures to palliate symptoms of advanced cancer were identified prospectively from all operations performed. Patients were observed for >90 days or until death.
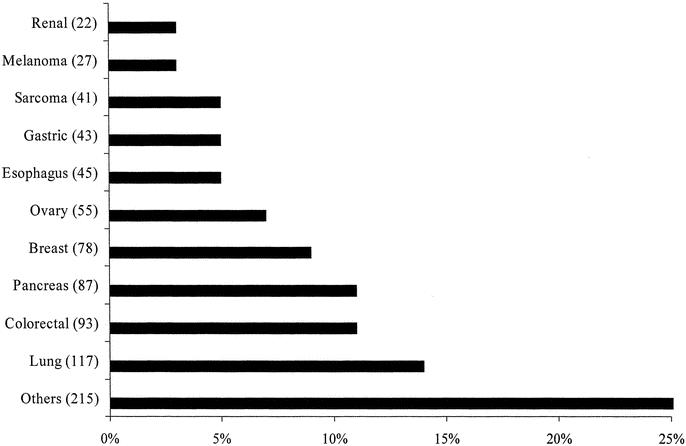
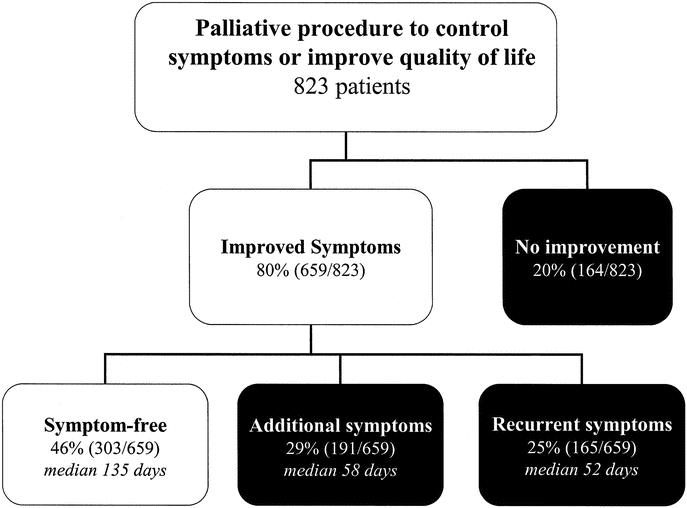
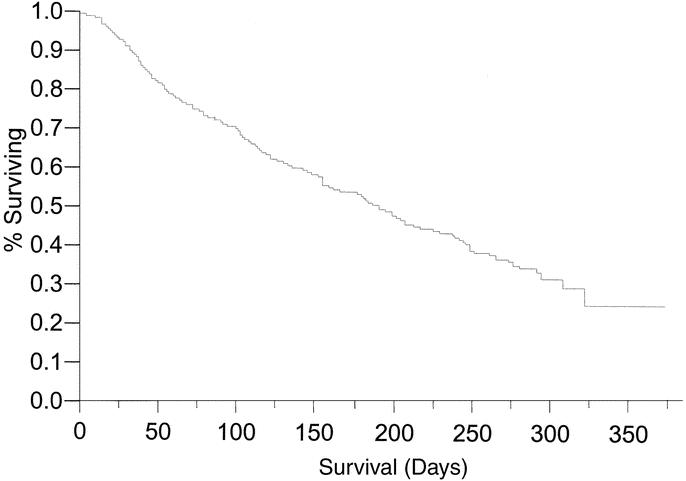
Results: There were 1022 palliative procedures performed in 823 patients from July 2002 to June 2003. Operative (713/1022) or endoscopic (309/1022) procedures were performed for gastrointestinal obstruction (34%), neurologic symptoms (23%), pain (12%), dyspnea (9%), jaundice (7%) or other symptoms (15%). Symptom improvement or resolution within 30 days was achieved in 80% (659/823). Median duration of symptom control was 135 days. Recurrence of the primary symptom occurred in 25% (165/659) while treatment of debilitating additional symptoms was required in 29% (191/659). Palliative procedures were associated with 30-day postoperative morbidity (29%) and mortality (11%). A major postoperative complication reduced the probability of symptom improvement to 17%. Median survival was 194 days from the time of the palliative procedure and was adversely associated with poor performance status (ECOG > or = 2 [P < 0.001] or NCI fatigue score of > or =1 [P < 0.001]), poor nutrition (albumin <3.5 [P = 0.005] or significant weight loss [P = 0.003]), and no previous cancer therapy (P = 0.002).
Conclusions: In carefully selected patients, relief of symptoms following palliative procedures can be expected, but new or recurrent symptoms limit durability. Potential benefits are minimized by postoperative complications and are less predictable for patients with poor performance status, malnutrition and no prior cancer therapy.
Figures
References
-
- Foley KM, Gelbrand H. Improving palliative care for cancer, Washington, DC: National Academy Press; 2001. - PubMed
-
- The American College of Surgeons Committee on Ethics. Statement on principles guiding care at the end of life. Bull Amer Col Surg. 1998;83:4. - PubMed
-
- Miner TJ, Jaques DP, Tavaf-Motamen H, et al. Decision making on surgical palliation based on patient outcome data. Amer J Surg. 1999;177:150–154. - PubMed
-
- Miner TJ, Jaques DP, Shriver CD. A prospective evaluation of patients undergoing surgery for the palliation of an advanced malignancy. Ann Surg Oncol. 2002;9:696–703. - PubMed
-
- McCahill LE, Krouse RS, Chu DZ, et al. Decision making in palliative surgery. JACS. 2002;195:411–422. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
