

Distribution of labelled anti-tenascin antibodies and fragments after injection into intact or partly resected C6-gliomas in rats
- PMID: 15449040
- PMCID: PMC11042174
- DOI: 10.1007/s00262-004-0608-7
Distribution of labelled anti-tenascin antibodies and fragments after injection into intact or partly resected C6-gliomas in rats
Abstract
Introduction: For treatment of malignant glioma, radioimmunotherapy has become a valuable alternative for more than 2 decades. Surprisingly, very little is known about the distribution of intralesionally administered labelled antibodies or fragments. We investigated the migration of labelled antibodies and antibody fragments injected into intact and partly resected C6-glioma in rats at different times after injection.
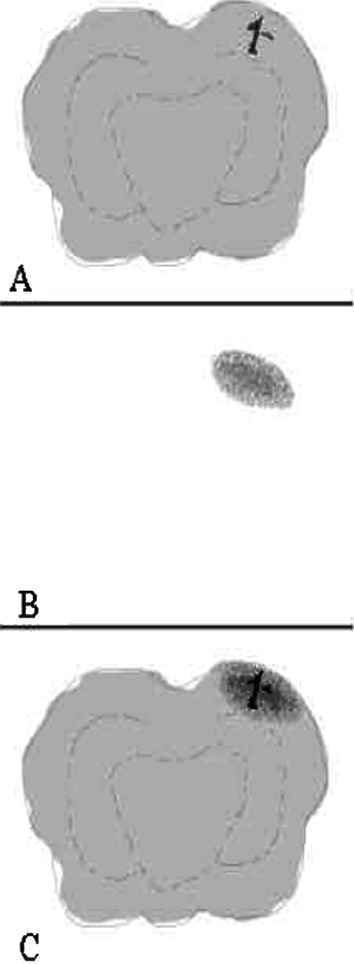
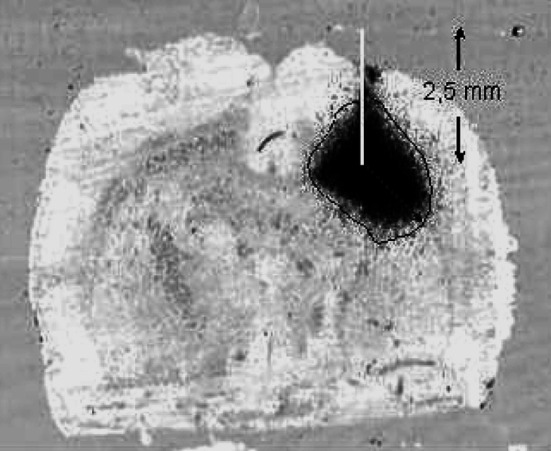
Materials and methods: Nine days after induction of a C6-glioma, 5 microl of 125I-labelled murine anti-tenascin antibodies (n = 31) or 125I-labelled fragments of anti-tenascin antibodies (n = 32) was injected slowly into the tumour (group I). In group II the tumour was subtotally resected 9 days after induction of the C6-glioma, and 24 h later the labelled antibodies (n = 30) or fragments (n = 12) were injected into the resection cavity. At 6, 24 or 48 h after the injection, animals were sacrificed, and brains removed. Distribution of labelled antibodies and fragments was determined by superimposing autoradiographs onto frozen sections and HE-stained neighbouring sections using a digital image analysing system.
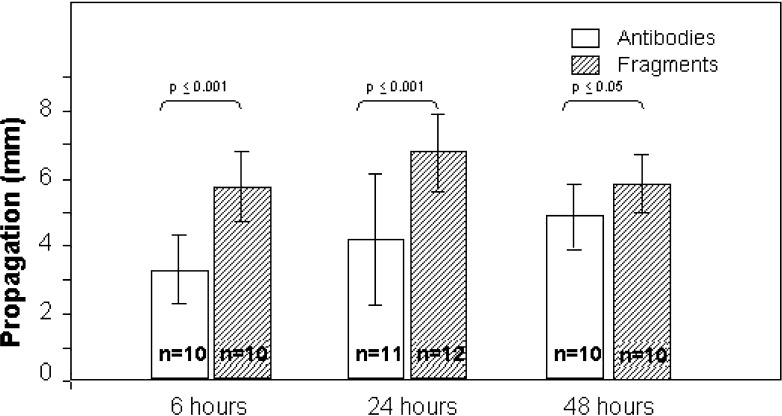
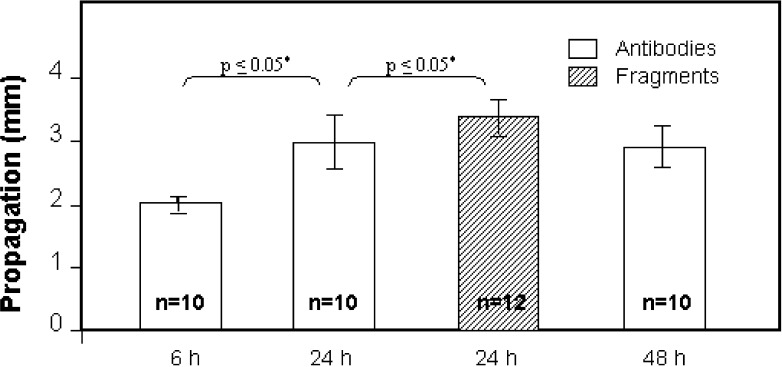
Results: After injection into intact C6-glioma, labelled antibodies covered a maximum distance of 3.2 +/- 1.0, 4.1 +/- 1.9 and 4.8 +/- 0.9 mm after 6, 24 and 48 h, respectively; while labelled fragments were found at a distance of 6.7 mm (+/-1.1) after 24 h and 5.8 mm (+/-0.9) after 48 h (significant in univariate analysis). Following partial tumour resection, the respective distances at 24 h were 3 +/- 0.4 mm for anti-tenascin antibodies and 3.4 +/- 0.3 mm for Fab fragments.
Conclusion: After injection into C6-glioma, labelled fragments are able to cover a greater distance than labelled antibodies. Injection of antibodies and fragments 1 day after tumour resection results in reduced velocity of both antibodies and fragments.
Figures

Similar articles
-
Intralesional radioimmunotherapy in the treatment of malignant glioma: clinical and experimental findings.Acta Neurochir Suppl. 2003;88:69-75. doi: 10.1007/978-3-7091-6090-9_12. Acta Neurochir Suppl. 2003. PMID: 14531564
-
Treatment of intracranial human glioblastoma by direct intratumoral administration of 131I-labelled anti-tenascin monoclonal antibody BC-2.Int J Cancer. 1992 Apr 22;51(1):7-13. doi: 10.1002/ijc.2910510103. Int J Cancer. 1992. PMID: 1373410
-
[Initial experiences with adjuvant locoregional radioimmunotherapy using 131I-labeled monoclonal antibodies against tenascin (BC-4) for treatment of glioma (WHO III and IV)].Nuklearmedizin. 2002 Jun;41(3):120-8. Nuklearmedizin. 2002. PMID: 12109031 German.
-
Antitenascin-C monoclonal antibody radioimmunotherapy for malignant glioma patients.Expert Rev Anticancer Ther. 2007 May;7(5):675-87. doi: 10.1586/14737140.7.5.675. Expert Rev Anticancer Ther. 2007. PMID: 17492931 Review.
-
Role of nuclear medicine in the treatment of malignant gliomas: the locoregional radioimmunotherapy approach.Eur J Nucl Med. 2000 May;27(5):601-9. doi: 10.1007/s002590050549. Eur J Nucl Med. 2000. PMID: 10853818 Review.
Cited by
-
Diffuse glioma growth: a guerilla war.Acta Neuropathol. 2007 Nov;114(5):443-58. doi: 10.1007/s00401-007-0293-7. Epub 2007 Sep 6. Acta Neuropathol. 2007. PMID: 17805551 Free PMC article. Review.
References
-
- Aaslid R, Groger U, Patlak CS, Fenstermacher JD, Huber P, Reulen HJ. Fluid flow rates in human peritumoural oedema. Acta Neurochir Suppl (Wien) 1990;51:152. - PubMed
-
- Albert FK, Forsting M, Sartor K, Adams HP, Kunze S. Early postoperative magnetic resonance imaging after resection of malignant glioma: objective evaluation of residual tumor and its influence on regrowth and prognosis. Neurosurgery. 1994;34:45. - PubMed
-
- Bashir R, Hochberg F, Oot R. Regrowth patterns of glioblastoma multiforme related to planning of interstitial brachytherapy radiation fields. Neurosurgery. 1988;23:27. - PubMed
-
- Behr TM, Wormann B, Gramatzki M, Riggert J, Gratz S, Behe M, Griesinger F, Sharkey RM, Kolb HJ, Hiddemann W, Goldenberg DM, Becker W. Low- versus high-dose radioimmunotherapy with humanized anti-CD22 or chimeric anti-CD20 antibodies in a broad spectrum of B cell-associated malignancies. Clin Cancer Res. 1999;5:3304s. - PubMed
-
- Bender H, Takahashi H, Adachi K, Belser P, Liang SH, Prewett M, Schrappe M, Sutter A, Rodeck U, Herlyn D. Immunotherapy of human glioma xenografts with unlabeled, 131I-, or 125I-labeled monoclonal antibody 425 to epidermal growth factor receptor. Cancer Res. 1992;52:121. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
