

Predicting the impact of a nonsterilizing vaccine against human immunodeficiency virus
- PMID: 15452255
- PMCID: PMC521856
- DOI: 10.1128/JVI.78.20.11340-11351.2004
Predicting the impact of a nonsterilizing vaccine against human immunodeficiency virus
Abstract
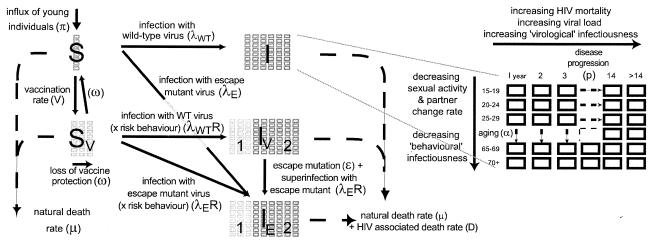
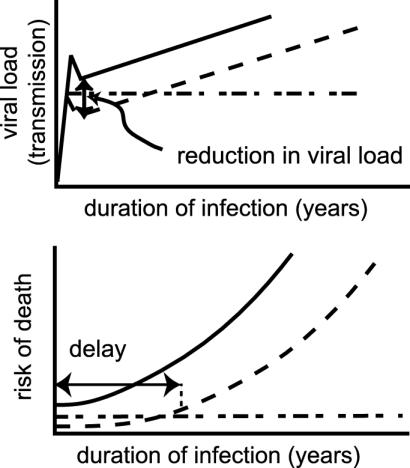
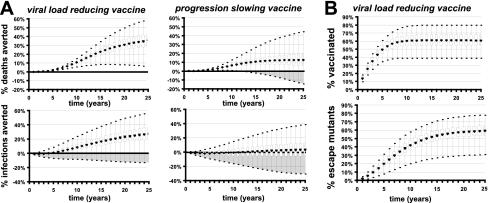
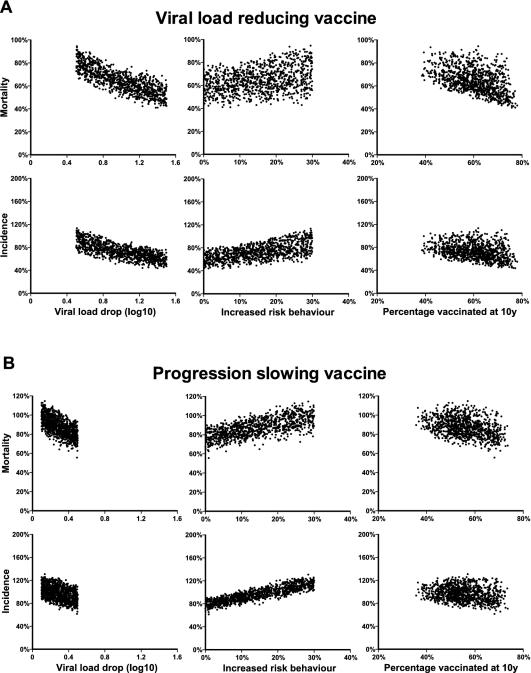
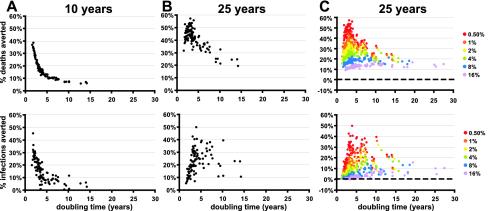
Studies of human immunodeficiency virus (HIV) vaccines in animal models suggest that it is difficult to induce complete protection from infection (sterilizing immunity) but that it is possible to reduce the viral load and to slow or prevent disease progression following infection. We have developed an age-structured epidemiological model of the effects of a disease-modifying HIV vaccine that incorporates the intrahost dynamics of infection, a transmission rate and host mortality that depend on the viral load, the possible evolution and transmission of vaccine escape mutant viruses, a finite duration of vaccine protection, and possible changes in sexual behavior. Using this model, we investigated the long-term outcome of a disease-modifying vaccine and utilized uncertainty analysis to quantify the effects of our lack of precise knowledge of various parameters. Our results suggest that the extent of viral load reduction in vaccinated infected individuals (compared to unvaccinated individuals) is the key predictor of vaccine efficacy. Reductions in viral load of about 1 log(10) copies ml(-1) would be sufficient to significantly reduce HIV-associated mortality in the first 20 years after the introduction of vaccination. Changes in sexual risk behavior also had a strong impact on the epidemic outcome. The impact of vaccination is dependent on the population in which it is used, with disease-modifying vaccines predicted to have the most impact in areas of low prevalence and rapid epidemic growth. Surprisingly, the extent to which vaccination alters disease progression, the rate of generation of escape mutants, and the transmission of escape mutants are predicted to have only a weak impact on the epidemic outcome over the first 25 years after the introduction of a vaccine.
Figures
Similar articles
-
Are Clade Specific HIV Vaccines a Necessity? An Analysis Based on Mathematical Models.EBioMedicine. 2015 Nov 5;2(12):2062-9. doi: 10.1016/j.ebiom.2015.11.009. eCollection 2015 Dec. EBioMedicine. 2015. PMID: 26844286 Free PMC article.
-
Estimating the benefit of an HIV-1 vaccine that reduces viral load set point.J Infect Dis. 2007 Feb 15;195(4):546-50. doi: 10.1086/510909. Epub 2007 Jan 5. J Infect Dis. 2007. PMID: 17230414
-
Expected epidemiological impact of the introduction of a partially effective HIV vaccine among men who have sex with men in Australia.Vaccine. 2011 Aug 18;29(36):6125-9. doi: 10.1016/j.vaccine.2011.06.061. Epub 2011 Jun 22. Vaccine. 2011. PMID: 21703320
-
Potential public health impact of imperfect HIV type 1 vaccines.J Infect Dis. 2005 Feb 1;191 Suppl 1:S85-96. doi: 10.1086/425267. J Infect Dis. 2005. PMID: 15627235 Review.
-
Molecular biological assessment methods and understanding the course of the HIV infection.APMIS Suppl. 2003;(114):1-37. APMIS Suppl. 2003. PMID: 14626050 Review.
Cited by
-
Herpes simplex virus as a tool to define the role of complement in the immune response to peripheral infection.Vaccine. 2008 Dec 30;26 Suppl 8(Suppl 8):I94-9. doi: 10.1016/j.vaccine.2008.11.062. Vaccine. 2008. PMID: 19388172 Free PMC article. Review.
-
Agent-based and phylogenetic analyses reveal how HIV-1 moves between risk groups: injecting drug users sustain the heterosexual epidemic in Latvia.Epidemics. 2012 Jun;4(2):104-16. doi: 10.1016/j.epidem.2012.04.002. Epub 2012 May 2. Epidemics. 2012. PMID: 22664069 Free PMC article.
-
Evolution of HIV virulence in response to disease-modifying vaccines: A modeling study.Vaccine. 2023 Oct 13;41(43):6461-6469. doi: 10.1016/j.vaccine.2023.08.071. Epub 2023 Sep 14. Vaccine. 2023. PMID: 37714749 Free PMC article.
-
The Effect of Interference on the CD8(+) T Cell Escape Rates in HIV.Front Immunol. 2015 Jan 13;5:661. doi: 10.3389/fimmu.2014.00661. eCollection 2014. Front Immunol. 2015. PMID: 25628620 Free PMC article.
-
Notwithstanding Circumstantial Alibis, Cytotoxic T Cells Can Be Major Killers of HIV-1-Infected Cells.J Virol. 2016 Jul 27;90(16):7066-7083. doi: 10.1128/JVI.00306-16. Print 2016 Aug 15. J Virol. 2016. PMID: 27226367 Free PMC article.
References
-
- Amara, R. R., F. Villinger, J. D. Altman, S. L. Lydy, S. P. O'Neil, S. I. Staprans, D. C. Montefiori, Y. Xu, J. G. Herndon, L. S. Wyatt, M. A. Candido, N. L. Kozyr, P. L. Earl, J. M. Smith, H. L. Ma, B. D. Grimm, M. L. Hulsey, J. Miller, H. M. McClure, J. M. McNicholl, B. Moss, and H. L. Robinson. 2001. Control of a mucosal challenge and prevention of AIDS by a multiprotein DNA/MVA vaccine. Science 292:69-74. - PubMed
-
- Anastos, K., L. A. Kalish, N. Hessol, B. Weiser, S. Melnick, D. Burns, R. Delapenha, J. DeHoVitz, M. Cohen, W. Meyer, J. Bremer, and A. Kovacs. 1999. The relative value of CD4 cell count and quantitative HIV-1 RNA in predicting survival in HIV-1-infected women: results of the women's interagency HIV study. AIDS 13:1717-1726. - PubMed
-
- Anderson, R. M., and G. P. Garnett. 1996. Low-efficacy HIV vaccines: potential for community-based intervention programmes. Lancet 348:1010-1013. - PubMed
-
- Anderson, R. M., S. Gupta, and R. M. May. 1991. Potential of community-wide chemotherapy or immunotherapy to control the spread of HIV-1. Nature 350:356-359. - PubMed
-
- Anderson, R. M., and R. M. May. 1991. Infectious diseases of humans. Oxford University Press, Oxford, United Kingdom.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
