

The fallacy of enrolling only high-risk subjects in cancer prevention trials: is there a "free lunch"?
- PMID: 15461821
- PMCID: PMC524373
- DOI: 10.1186/1471-2288-4-24
The fallacy of enrolling only high-risk subjects in cancer prevention trials: is there a "free lunch"?
Abstract
Background: There is a common belief that most cancer prevention trials should be restricted to high-risk subjects in order to increase statistical power. This strategy is appropriate if the ultimate target population is subjects at the same high-risk. However if the target population is the general population, three assumptions may underlie the decision to enroll high-risk subject instead of average-risk subjects from the general population: higher statistical power for the same sample size, lower costs for the same power and type I error, and a correct ratio of benefits to harms. We critically investigate the plausibility of these assumptions.
Methods: We considered each assumption in the context of a simple example. We investigated statistical power for fixed sample size when the investigators assume that relative risk is invariant over risk group, but when, in reality, risk difference is invariant over risk groups. We investigated possible costs when a trial of high-risk subjects has the same power and type I error as a larger trial of average-risk subjects from the general population. We investigated the ratios of benefit to harms when extrapolating from high-risk to average-risk subjects.
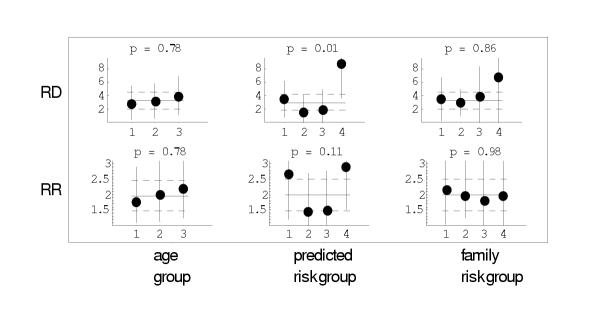
Results: Appearances here are misleading. First, the increase in statistical power with a trial of high-risk subjects rather than the same number of average-risk subjects from the general population assumes that the relative risk is the same for high-risk and average-risk subjects. However, if the absolute risk difference rather than the relative risk were the same, the power can be less with the high-risk subjects. In the analysis of data from a cancer prevention trial, we found that invariance of absolute risk difference over risk groups was nearly as plausible as invariance of relative risk over risk groups. Therefore a priori assumptions of constant relative risk across risk groups are not robust, limiting extrapolation of estimates of benefit to the general population. Second, a trial of high-risk subjects may cost more than a larger trial of average risk subjects with the same power and type I error because of additional recruitment and diagnostic testing to identify high-risk subjects. Third, the ratio of benefits to harms may be more favorable in high-risk persons than in average-risk persons in the general population, which means that extrapolating this ratio to the general population would be misleading. Thus there is no free lunch when using a trial of high-risk subjects to extrapolate results to the general population.
Conclusion: Unless the intervention is targeted to only high-risk subjects, cancer prevention trials should be implemented in the general population.
Figures
References
-
- Gail MH, Brinton LA, Byar DP, Corle DK, Green SB, Schairer C, Mulvihill JJ. Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. Journal of the National Cancer Institute. 1989;81:1879–1886. doi: 10.1093/jnci/81.24.1879. - DOI - PubMed
-
- Frideman LM, Furberg CD, DeMets DL. Fundamental of Clinical Trials. John Wright: Boston; 1981.
-
- Baker SG, Freedman LS. Potential impact of genetic testing on cancer prevention trials, using breast cancer as an example. Journal of the National Cancer Institute. 1995;87:1137–1144. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
