

Renal outcome in adults with renal insufficiency and irregular asymmetric kidneys
- PMID: 15462683
- PMCID: PMC526254
- DOI: 10.1186/1471-2369-5-12
Renal outcome in adults with renal insufficiency and irregular asymmetric kidneys
Abstract
Background: The commonest cause of end-stage renal failure (ESRF) in children and young adults is congenital malformation of the kidney and urinary tract. In this retrospective review, we examine whether progression to ESRF can be predicted and whether treatment with angiotensin converting enzyme inhibitors (ACEI) can delay or prevent this.
Methods: We reviewed 78 patients with asymmetric irregular kidneys as a consequence of either primary vesico-ureteric reflux or renal dysplasia (Group 1, n = 44), or abnormal bladder function (Group 2, n = 34). Patients (median age 24 years) had an estimated GFR (eGFR) < 60 ml/min/1.73 m2 with at least 5 years of follow up (median 143 months). 48 patients received ACEI. We explored potential prognostic factors that affect the time to ESRF using Cox-regression analyses.
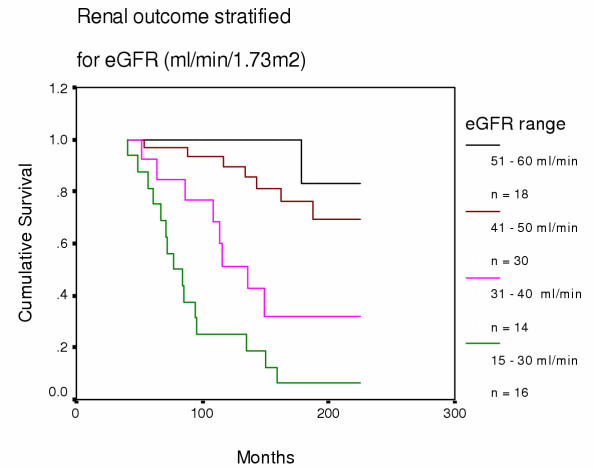
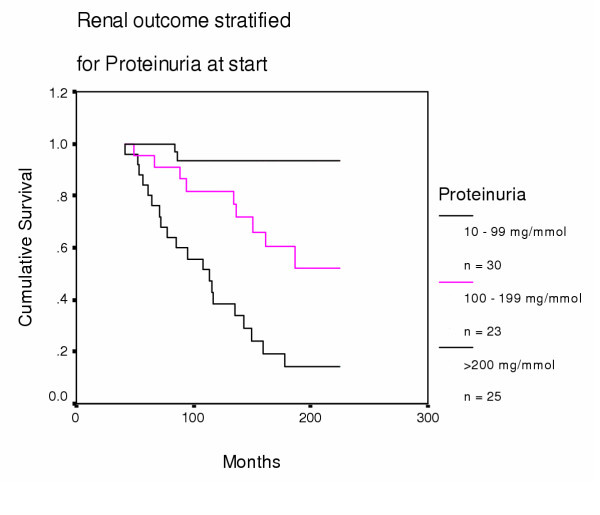
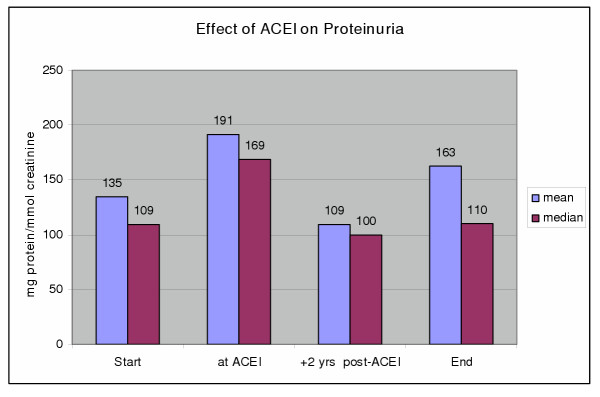
Results: At start, mean (SE) creatinine was 189 (8) mumol/l, mean eGFR 41 (1) ml/min 1.73 m2, mean proteinuria 144 (14) mg/mmol creatinine (1.7 g/24 hrs). Of 78 patients, 36 (46%) developed ESRF, but none of 19 with proteinuria less than 50 mg/mmol and only two of 18 patients with eGFR above 50 ml/min did so. Renal outcome between Groups 1 and 2 appeared similar with no evidence for a difference. A benefit in favour of treatment with ACEI was observed above an eGFR of 40 ml/min (p = 0.024).
Conclusion: The similar outcome of the two groups supports the nephrological nature of progressive renal failure in young men born with abnormal bladders. There is a watershed GFR of 40-50 ml/min at which ACEI treatment can be successful at improving renal outcome.
Figures
References
-
- Ansell D, FeestTG and Byrne C, editor. The UK Renal Registry 5th Annual Report. 2002. British Association for Paediatric Nephrology. Report from the Paediatric Renal Registry; pp. 253–273.
-
- Arze RS, Ramos JM, Owen JP, Morley AR, Elliott RW, Wilkinson R, Ward MK, Kerr DN. The natural history of chronic pyelonephritis in the adult. Q J Med. 1982;51:396–410. - PubMed
-
- el Khatib MT, Becker GJ, Kincaid-Smith PS. Reflux nephropathy and primary vesicoureteric reflux in adults. Q J Med. 1990;77:1241–1253. - PubMed
-
- Zhang Y, Bailey RR. A long term follow up of adults with reflux nephropathy. N Z Med J. 1995;108:142–144. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
