

Radiofrequency ablation of liver cancer: early evaluation of therapeutic response with contrast-enhanced ultrasonography
- PMID: 15467416
- PMCID: PMC2698161
- DOI: 10.3348/kjr.2004.5.3.185
Radiofrequency ablation of liver cancer: early evaluation of therapeutic response with contrast-enhanced ultrasonography
Abstract
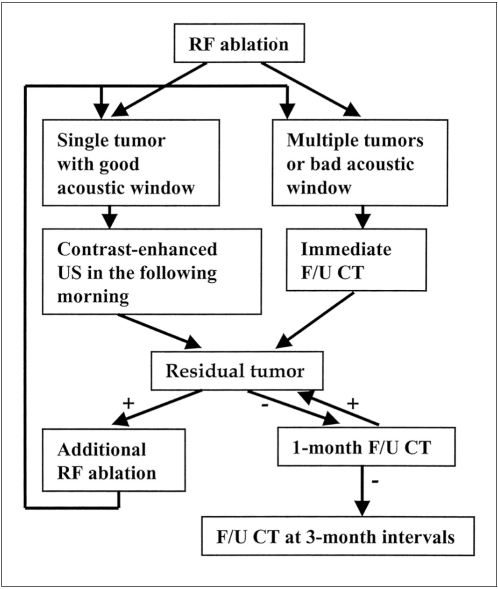
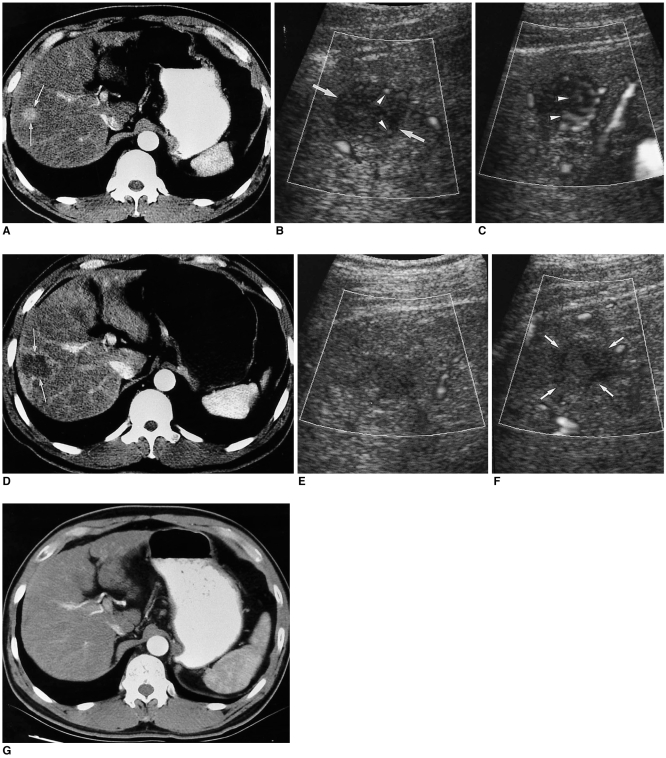
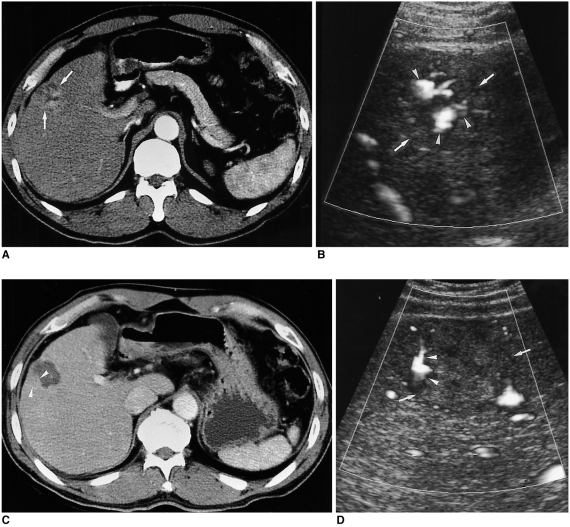
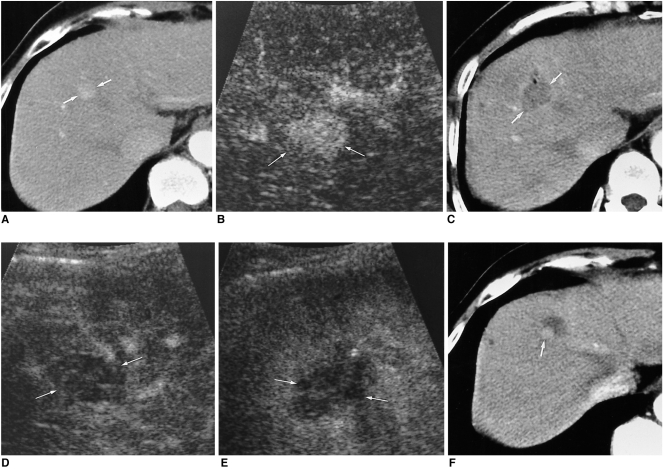
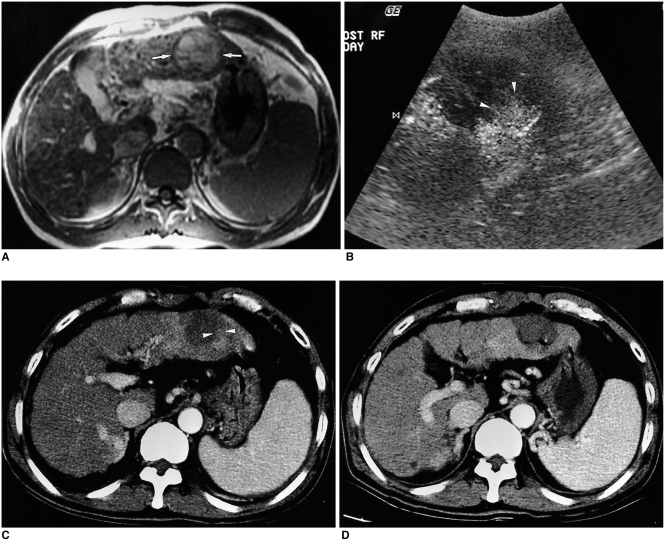
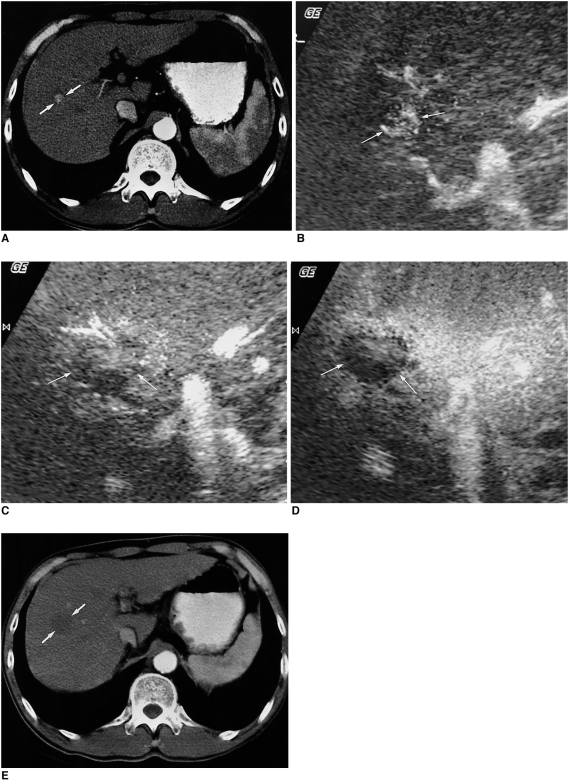
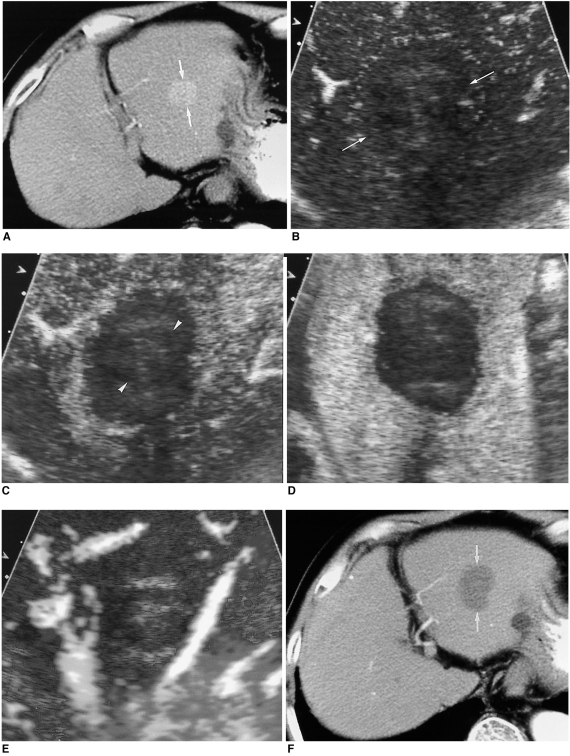
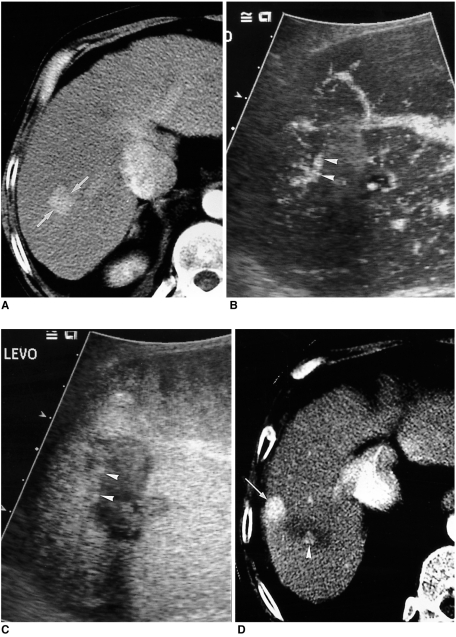
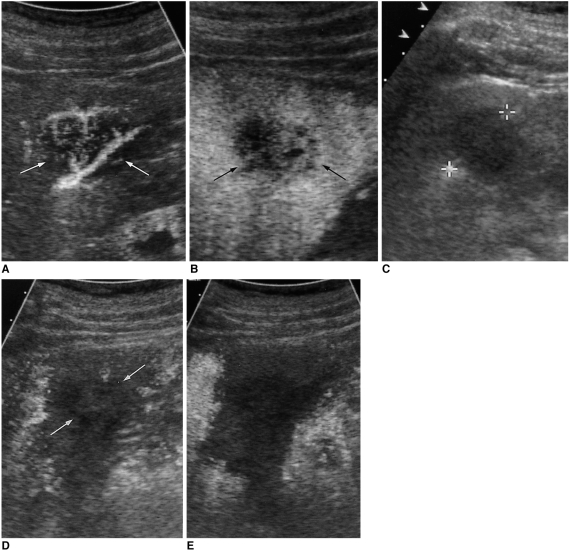
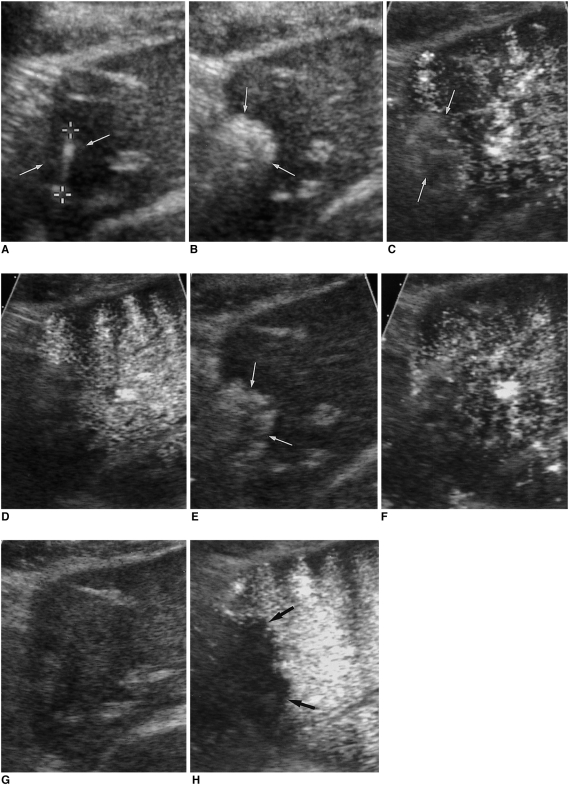
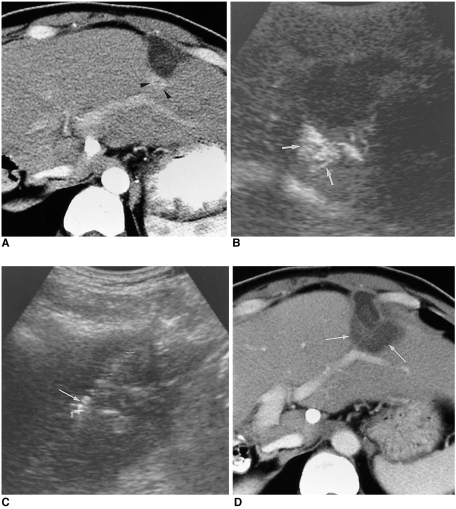
The early assessment of the therapeutic response after percutaneous radiofrequency (RF) ablation is important, in order to correctly decide whether further treatment is necessary. The residual unablated tumor is usually depicted on contrast-enhanced multiphase helical computed tomography (CT) as a focal enhancing structure during the arterial and portal venous phases. Contrast-enhanced color Doppler and power Doppler ultrasonography (US) have also been used to detect residual tumors. Contrast-enhanced gray-scale US, using a harmonic technology which has recently been introduced, allows for the detection of residual tumors after ablation, without any of the blooming or motion artifacts usually seen on contrast-enhanced color or power Doppler US. Based on our experience and reports in the literature, we consider that contrast-enhanced gray-scale harmonic US constitutes a reliable alternative to contrast-enhanced multiphase CT for the early evaluation of the therapeutic response to RF ablation for liver cancer. This technique was also useful in targeting any residual unablated tumors encountered during additional ablation.
Figures
Similar articles
-
Therapeutic response assessment of percutaneous radiofrequency ablation for hepatocellular carcinoma: utility of contrast-enhanced agent detection imaging.Eur J Radiol. 2005 Oct;56(1):66-73. doi: 10.1016/j.ejrad.2005.03.023. Eur J Radiol. 2005. PMID: 15913940 Clinical Trial.
-
Hepatocellular carcinoma treated with percutaneous radio-frequency ablation: usefulness of power Doppler US with a microbubble contrast agent in evaluating therapeutic response-preliminary results.Radiology. 2000 Nov;217(2):558-63. doi: 10.1148/radiology.217.2.r00oc07558. Radiology. 2000. PMID: 11058660
-
Early assessment of the therapeutic response to radio frequency ablation for hepatocellular carcinoma: utility of gray scale harmonic ultrasonography with a microbubble contrast agent.J Ultrasound Med. 2003 Nov;22(11):1163-72. doi: 10.7863/jum.2003.22.11.1163. J Ultrasound Med. 2003. PMID: 14620886
-
Hepatocellular carcinoma treated with radio-frequency ablation: spectrum of imaging findings.Radiographics. 2003 Jan-Feb;23(1):107-21. doi: 10.1148/rg.231025055. Radiographics. 2003. PMID: 12533646 Review.
-
[Hepatocellular carcinoma: Role of imaging diagnostics in detection, intervention and follow-up].Rofo. 2002 Nov;174(11):1358-68. doi: 10.1055/s-2002-35349. Rofo. 2002. PMID: 12424661 Review. German.
Cited by
-
Sonography guided percutaneous radiofrequency ablation of hepatocellular carcinoma: effect of cooperative training on the pretreatment assessment of the operation's feasibility.Korean J Radiol. 2008 Jan-Feb;9(1):29-37. doi: 10.3348/kjr.2008.9.1.29. Korean J Radiol. 2008. PMID: 18253073 Free PMC article.
-
Percutaneous radiofrequency ablation for early-stage hepatocellular carcinoma as a first-line treatment: long-term results and prognostic factors in a large single-institution series.Eur Radiol. 2007 Mar;17(3):684-92. doi: 10.1007/s00330-006-0461-5. Epub 2006 Nov 9. Eur Radiol. 2007. PMID: 17093964
-
Contrast enhanced ultrasound of hepatocellular carcinoma.World J Radiol. 2010 Feb 28;2(2):68-82. doi: 10.4329/wjr.v2.i2.68. World J Radiol. 2010. PMID: 21160920 Free PMC article.
References
-
- Dodd GD, 3rd, Soulen MC, Kane RA, et al. Minimally invasive treatment of malignant hepatic tumors: at the threshold of a major breakthrough. RadioGraphics. 2000;20:9–27. - PubMed
-
- Livraghi T, Goldberg SN, Lazzarni S, Meloni F, Solbiati L, Gazelle GS. Small hepatocellular carcinoma: treatment with radio-frequency ablation versus ethanol injection. Radiology. 1999;210:655–661. - PubMed
-
- Gazelle GS, Goldberg SN, Solbiati L, Livraghi T. Tumor ablation with radio-frequency energy. Radiology. 2000;217:633–646. - PubMed
-
- McGahan JP, Dodd GD., 3rd Radiofrequency ablation of the liver: current status. AJR Am J Roentgenol. 2001;176:3–16. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
