

The effectiveness of five strategies for the prevention of gastrointestinal toxicity induced by non-steroidal anti-inflammatory drugs: systematic review
- PMID: 15475342
- PMCID: PMC524106
- DOI: 10.1136/bmj.38232.680567.EB
The effectiveness of five strategies for the prevention of gastrointestinal toxicity induced by non-steroidal anti-inflammatory drugs: systematic review
Abstract
Objectives: To assess the effectiveness of five gastroprotective strategies for people taking non-steroidal anti-inflammatory drugs (NSAIDs)--H2 receptor antagonists plus non-selective (or cyclo-oxygenase-1) NSAIDs; proton pump inhibitors plus non-selective NSAIDs; misoprostol plus non-selective NSAIDs; COX-2 selective NSAIDs; or COX-2 specific NSAIDs--in reducing serious gastrointestinal complications, symptomatic ulcers, serious cardiovascular or renal disease, and deaths, and improving quality of life.
Data sources: The Cochrane Library, Medline, Embase, Current Controlled Trials, and System for Information on Grey Literature in Europe (SIGLE) were searched to May 2002. Bibliographies and author contacts were used to identify further studies; non-English articles were included.
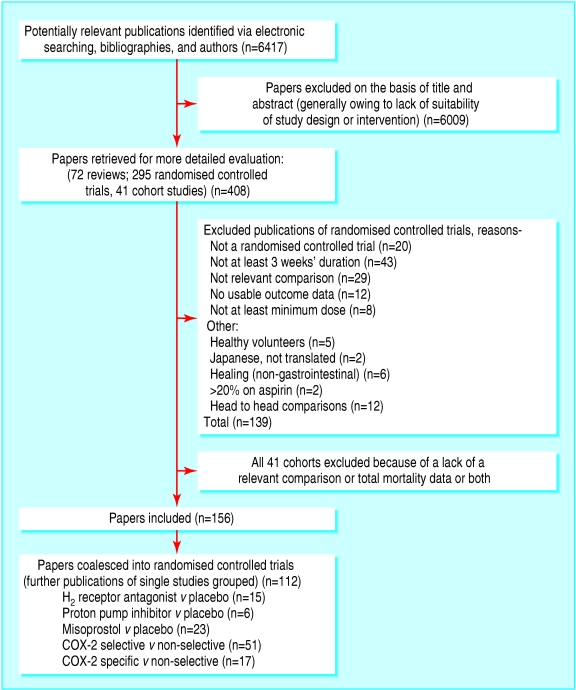
Review methods: Trial selection, data extraction, and quality assessment were performed independently, in duplicate. Articles were rejected only if the study was not a randomised controlled trial; did not assess a gastroprotective strategy versus placebo; included exclusively children or healthy volunteers; lasted less than 21 days; or no review outcomes were measured. Quality assessment included allocation concealment and baseline similarity. Random effects meta-analysis, meta-regression and subgrouping were used to pool effects and analyse associations with length of follow up, mean age, and baseline gastrointestinal status. Heterogeneity was examined and sensitivity analyses performed.
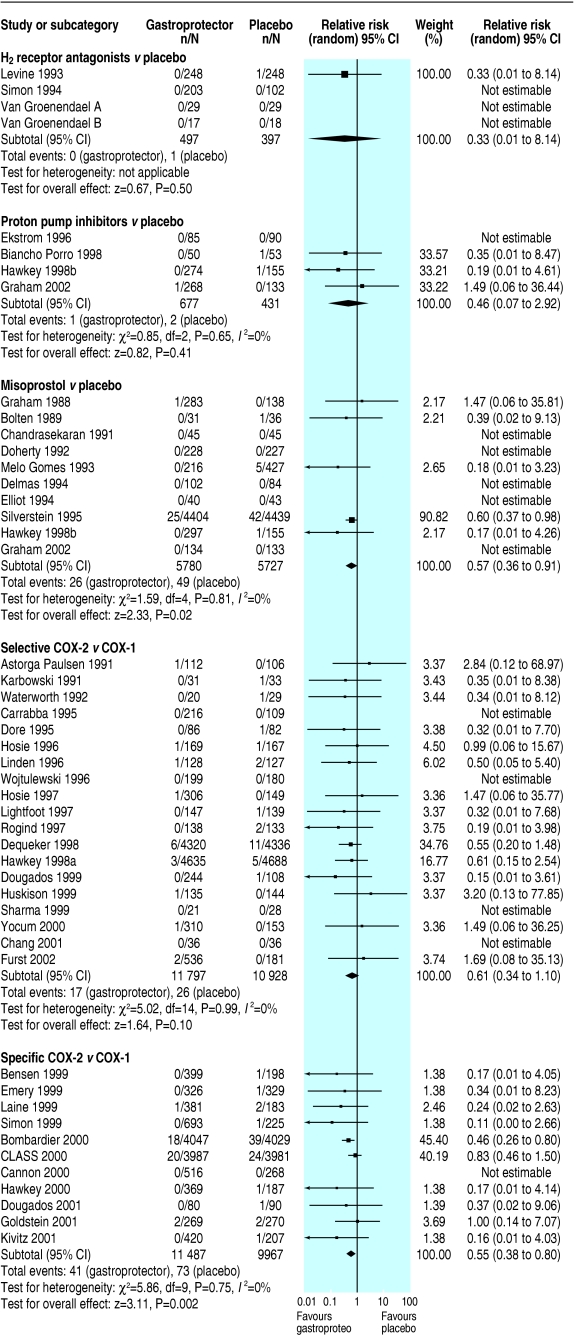
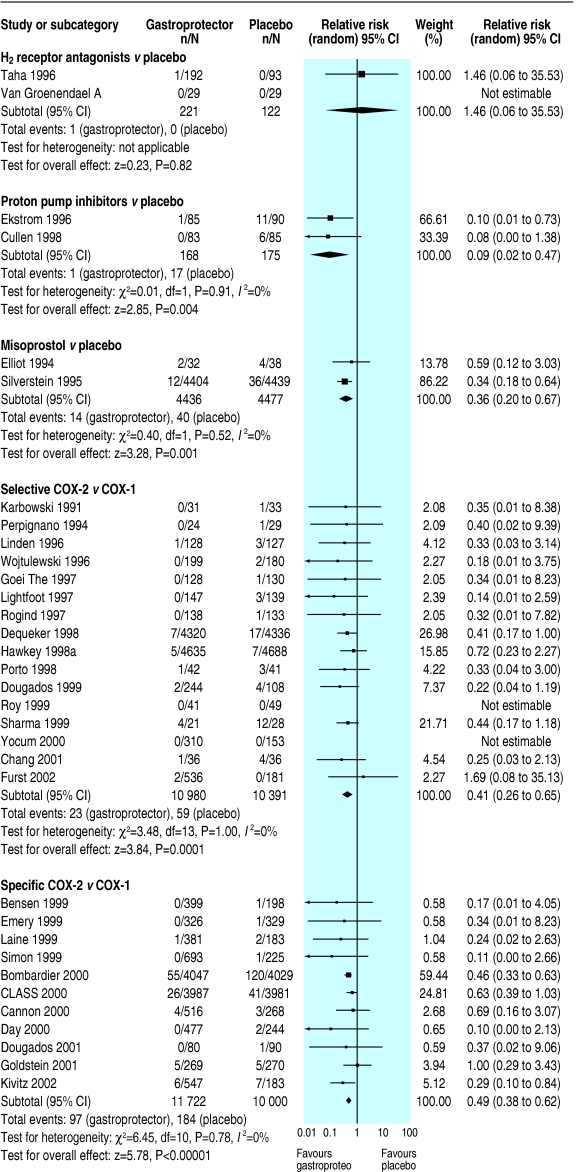
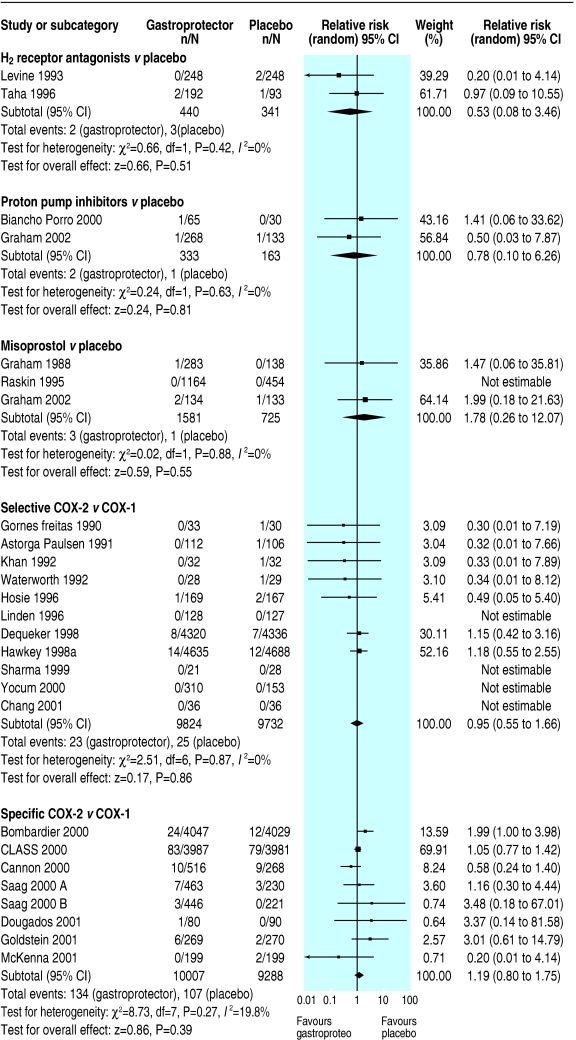
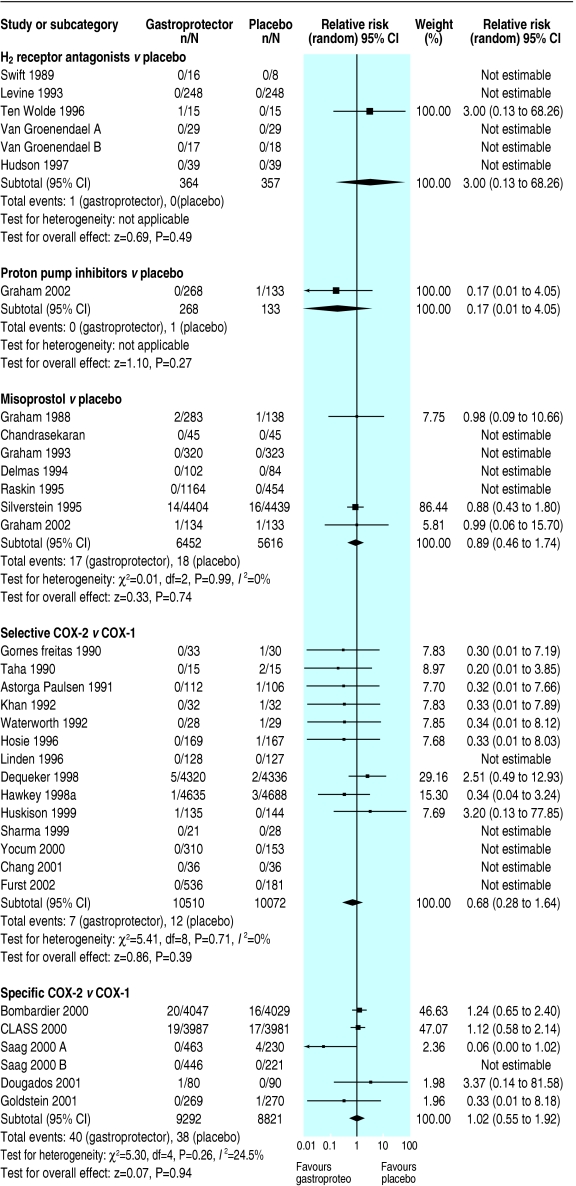
Results: Of 112 included randomised controlled trials (74 666 participants), five were judged to be at low risk of bias, and 138 deaths and 248 serious gastrointestinal events were reported overall. On comparing gastroprotective strategies versus placebo we found no evidence of effectiveness of H2 receptor antagonists for any primary outcomes (few events reported); proton pump inhibitors may reduce the risk of symptomatic ulcers (relative risk 0.09, 95% confidence interval 0.02 to 0.47); misoprostol reduces the risk of serious gastrointestinal complications (0.57, 0.36 to 0.91) and symptomatic ulcers (0.36, 0.20 to 0.67); COX-2 selectives reduce the risk of symptomatic ulcers (0.41, 0.26 to 0.65) and COX-2 specifics reduce the risk of symptomatic ulcers (0.49, 0.38 to 0.62) and possibly serious gastrointestinal complications (0.55, 0.38 to 0.80). All strategies except COX-2 selectives reduce the risk of endoscopic ulcers (at least 3 mm in diameter).
Conclusions: Misoprostol, COX-2 specific and selective NSAIDs, and probably proton pump inhibitors significantly reduce the risk of symptomatic ulcers, and misoprostol and probably COX-2 specifics significantly reduce the risk of serious gastrointestinal complications, but data quality is low. More data on H2 receptor antagonists and proton pump inhibitors are needed, as is better reporting of rare but important outcomes.
Figures
Comment in
-
Review: misoprostol or COX-2-specific or selective NSAIDs reduce gastrointestinal complications and symptomatic ulcers.ACP J Club. 2005 May-Jun;142(3):75. ACP J Club. 2005. PMID: 15862074 No abstract available.
References
-
- National Institute for Clinical Excellence. Guidance on the use of cyclo-oxygenase (COX) II selective inhibitors, celecoxib, rofecoxib, meloxicam, and etodolac for osteoarthritis and rheumatoid arthritis. London, NICE: 2001. (Technology Appraisal Guidance, 27.)
-
- Blower AL, Brooks A, Fenn GC, Hill A, Pearce MY, Morant S, et al. Emergency admissions for upper gastrointestinal disease and their relation to NSAID use. Aliment Pharmacol Ther 1997;11: 283-91. - PubMed
-
- Eversmeyer W, Poland M, DeLapp RE, Jensen CP. Safety experience with nabumetone versus diclofenac, naproxen, ibuprofen, and piroxicam in osteoarthritis and rheumatoid arthritis. Am J Med 1993;95: 10S-8S. - PubMed
-
- Lister BJ, Poland M, DeLapp RE. Efficacy of nabumetone versus diclofenac, naproxen, ibuprofen, and piroxicam in osteoarthritis and rheumatoid arthritis. Am J Med 1993;95: 2S-9S. - PubMed
-
- Rostom A, Dube C, Wells G, Tugwell P, Welch V, Jolicoeur E, et al. Prevention of NSAID-induced gastroduodenal ulcers. Cochrane Database Syst Rev 2002;(4): CD002296. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials