

Brain functional magnetic resonance imaging of rectal pain and activation of endogenous inhibitory mechanisms in irritable bowel syndrome patient subgroups and healthy controls
- PMID: 15479679
- PMCID: PMC1774298
- DOI: 10.1136/gut.2003.028514
Brain functional magnetic resonance imaging of rectal pain and activation of endogenous inhibitory mechanisms in irritable bowel syndrome patient subgroups and healthy controls
Abstract
Background and aims: Many patients with irritable bowel syndrome (IBS) show intestinal hypersensitivity to distension and sensitisation after repeated intestinal distensions. Abnormalities in endogenous pain inhibitory mechanisms, such as diffuse noxious inhibitory controls (DNIC), may be implicated and were investigated during brain functional magnetic resonance imaging (fMRI).
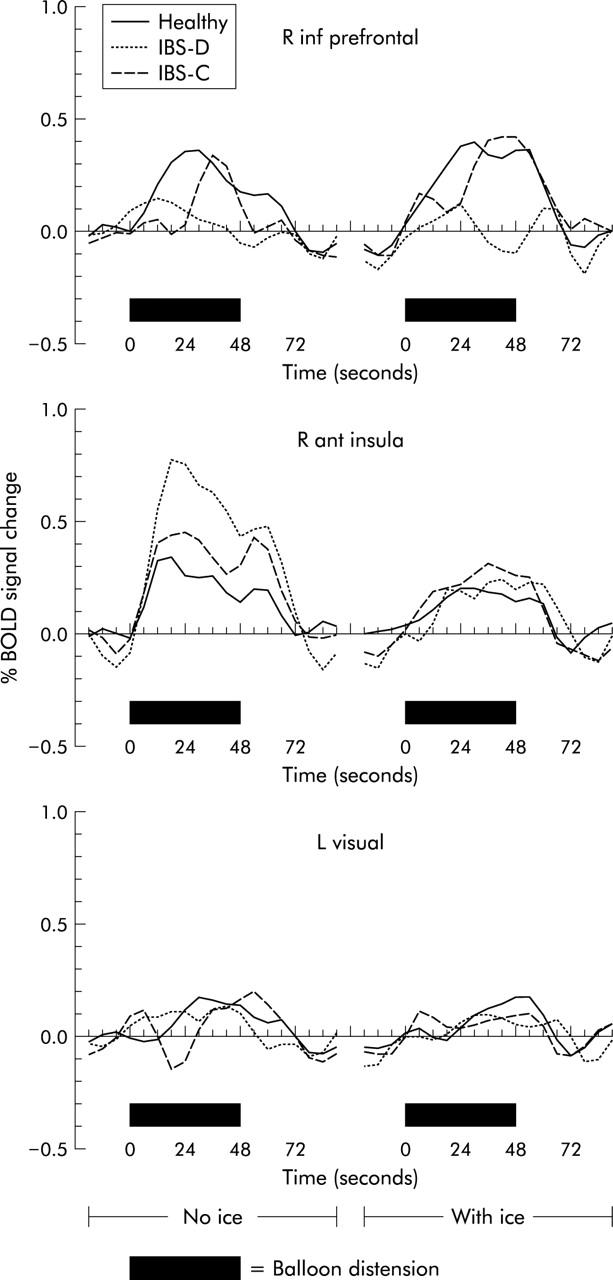
Patients and methods: fMRI was performed in 10 female patients with IBS (five constipated (IBS-C) and five with diarrhoea (IBS-D)) and 10 female healthy controls during rectal balloon distension alone or during activation of DNIC by painful heterotopic stimulation of the foot with ice water. Rectal pain was scored with and without heterotopic stimulation (0 = none, 10 = maximal).
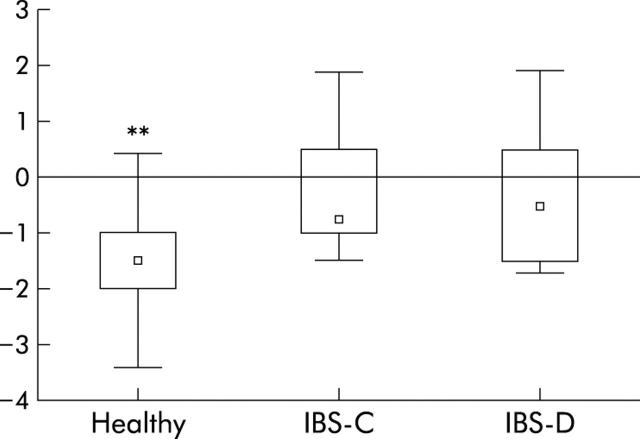
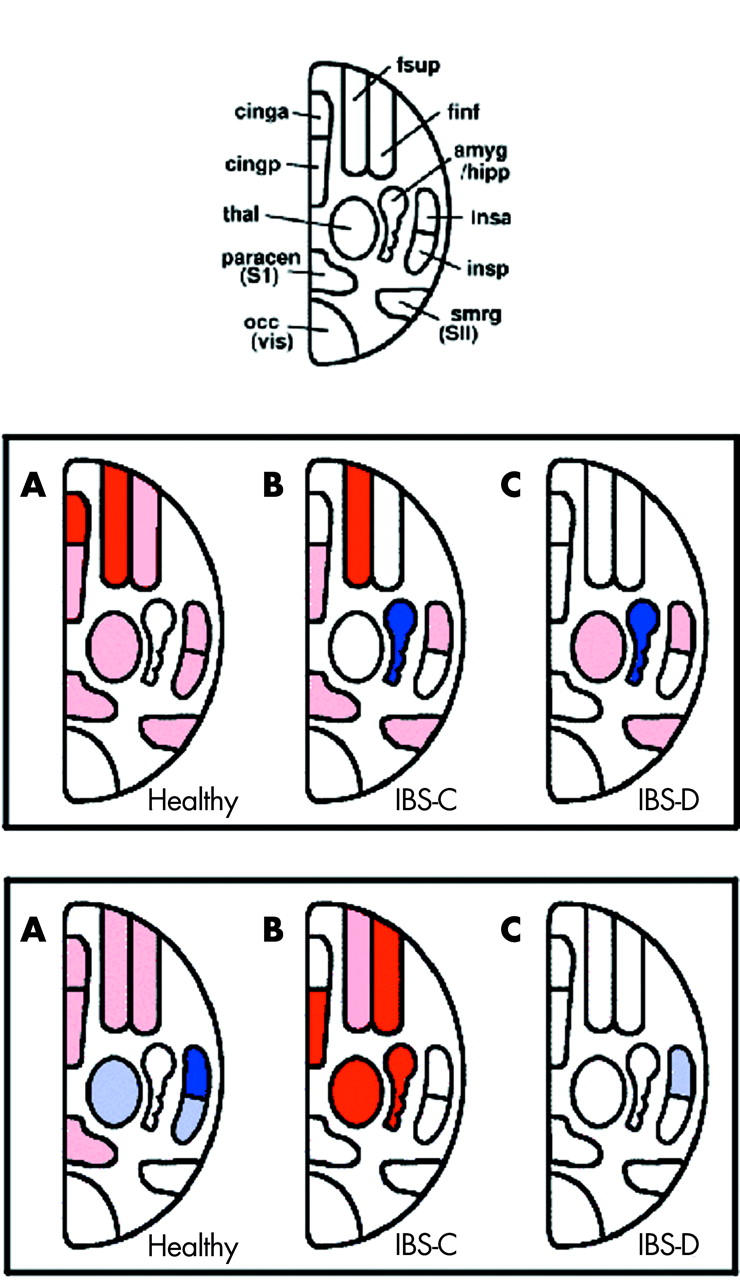
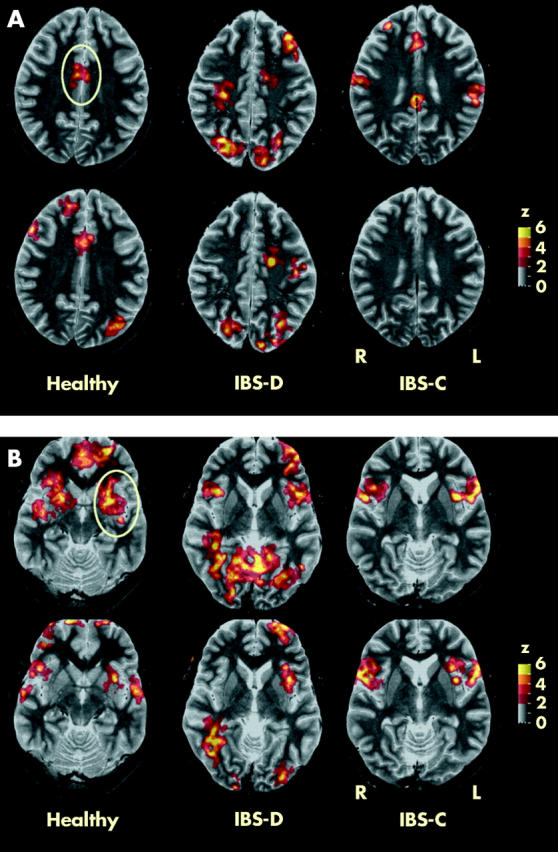
Results: Heterotopic stimulation decreased median rectal pain scores significantly in healthy controls (-1.5 (interquartile range -2 to -1); p = 0.001) but not in IBS-C (-0.7 (-1 to 0.5)), IBS-D (-0.5 (-1.5 to 0.5)), or in all IBS patients (0 (-1.5 to 1.3)). Brain activation changes during heterotopic stimulation differed highly significantly between IBS-C, IBS-D, and controls. The main centres affected were the amygdala, anterior cingulate cortex, hippocampus, insula, periaqueductal gray, and prefrontal cortex, which form part of the matrix controlling emotional, autonomic, and descending modulatory responses to pain.
Conclusions: IBS-C and IBS-D appear to have differing abnormal endogenous pain inhibitory mechanisms, involving DNIC and other supraspinal modulatory pathways.
Figures
Comment in
-
Importance of anti- and pro-nociceptive mechanisms in human disease.Gut. 2004 Nov;53(11):1553-5. doi: 10.1136/gut.2004.046110. Gut. 2004. PMID: 15479668 Free PMC article. Review. No abstract available.
References
-
- Drossman DA, Corazziari E, Talley NJ, et al. The functional gastrointestinal disorders. McLean: Degnon Associates, 2000:355–362.
-
- Whitehead WE, Engel BT, Schuster MM. Irritable bowel syndrome: physiological and psychological differences between diarrhoea-predominant and constipation-predominant patients. Dig Dis Sci 1980;25:404–13. - PubMed
-
- Sun WM, Read NW, Prior A, et al. Sensory and motor responses to rectal distension vary according to rate and pattern of balloon inflation. Gastroenterology 1990;99:1008–15. - PubMed
-
- Hasler WL, Soudah HC, Owyang C. Somatostatin analog inhibits afferent response to rectal distension in diarrhoea-predominant irritable bowel patients. J Pharmacol Exp Ther 1994;268:1206–11. - PubMed
-
- Hammer J , Phillips SF, Talley NJ, et al. Effect of a 5-HT3 antagonist (ondansetron) on rectal contractility and compliance in health and the irritable bowel syndrome. Aliment Pharmacol Ther 1993;7:543–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical