

Induction of T lymphocyte apoptosis by sulphasalazine in patients with Crohn's disease
- PMID: 15479684
- PMCID: PMC1774288
- DOI: 10.1136/gut.2003.037911
Induction of T lymphocyte apoptosis by sulphasalazine in patients with Crohn's disease
Abstract
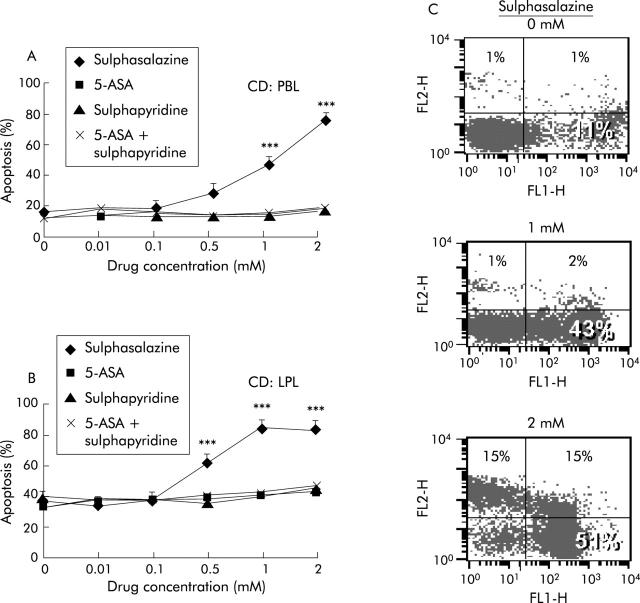
Background: Lamina propria T lymphocytes (LPL) of the intestinal mucosa are chronically activated in Crohn's disease (CD). Defective apoptosis of activated LPL was proposed as a key pathogenic mechanism. In fact, increased expression of antiapoptotic molecules was observed in CD LPL. In the present work, we aimed to analyse the effects and underlying molecular mechanisms of 5-amino salicylic acid (5-ASA) and derivatives on apoptosis of LPL and peripheral blood lymphocytes (PBL) in patients with CD compared with ulcerative colitis (UC) and in non-inflammatory controls.
Methods: PBL and LPL were isolated by Ficoll-Hypopaque gradient centrifugation and the EGTA-collagenase method, respectively. PBL/LPL were stimulated with FasL, 5-ASA, sulphapyridine, and sulphasalazine for 24/48 hours and apoptosis was quantified by flow cytometry (annexin V- propidium iodide method) and immunofluorescence. The molecular mechanisms of drug induced apoptosis were analysed in wild-type and FADD-/- Jurkat T cells using western blots and caspase assays.
Results: While PBL displayed a normal apoptosis pattern after Fas stimulation in patients with active CD, LPL from inflammatory areas were highly resistant. Comparable resistance to apoptosis was observed in LPL of UC patients. In contrast with 5-ASA, which did not induce apoptosis in lymphocytes, sulphasalazine proved to be a potent proapoptotic agent. Sulphasalazine induced T lymphocyte apoptosis was independent of the Fas pathway but associated with marked downregulation of antiapoptotic bcl-xl and bcl2, activation of the mitochondrial apoptosis signalling pathway, and subsequent activation of caspase-9 and caspase-3.
Conclusion: The beneficial effect of sulphasalazine in treating inflammatory bowel disease is at least in part attributable to its proapoptotic effects on LPL which allows potent downregulation of lymphocyte activation.
Figures



Comment in
-
T cell apoptosis and inflammatory bowel disease.Gut. 2004 Nov;53(11):1556-8. doi: 10.1136/gut.2004.040824. Gut. 2004. PMID: 15479669 Free PMC article. Review. No abstract available.
References
-
- Fiocchi C . Inflammatory bowel disease: etiology and pathogenesis. Gastroenterology 1998;115:182–205. - PubMed
-
- Podolsky DK. Inflammatory bowel disease. N Engl J Med 2002;347:417–29. - PubMed
-
- Shanahan F . Crohn’s disease. Lancet 2002;359:62–9. - PubMed
-
- Levine AD. Apoptosis: Implications for inflammatory bowel disease. IBD 2000;6:191–205. - PubMed
-
- Ina K , Itoh J, Fukushima K, et al. Resistance of Crohn’s disease T cells to multiple apoptotic signals is associated with a Bcl-2/Bax mucosal imbalance. J Immunol 1999;163:1081–90. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous