

Review
doi: 10.1136/gut.2003.015511.
Value of genetic testing in the management of pancreatitis
Affiliations
- PMID: 15479696
- PMCID: PMC1774302
- DOI: 10.1136/gut.2003.015511
Item in Clipboard
Review
Value of genetic testing in the management of pancreatitis
Gut.
2004 Nov.
No abstract available
Figures
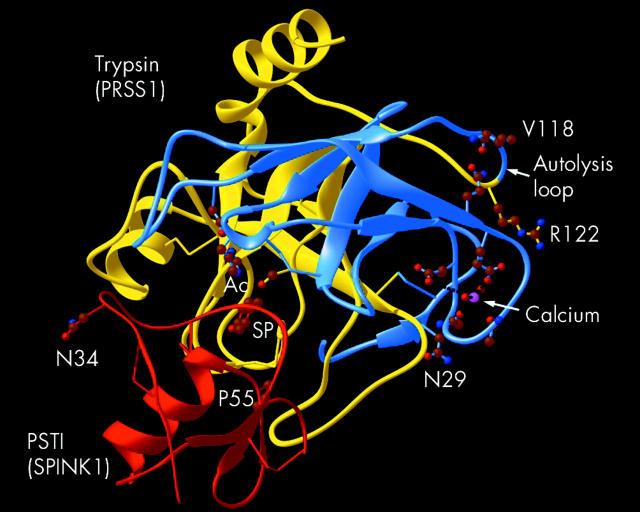
Structural features of trypsin (PRSS1) and PSTI (SPINK1). Residues in cationic trypsin (PRSS1 gene–blue and yellow) include the active catalytic site (Ac), R122, and V118 within the autolysis loop, the calcium binding loop with calcium (pink), and the residue interacting with V118 of the autolysis loop. N29 is shown near the activation site. In the PSTI (SPINK1 gene–Red), N34 and P55 are shown and residue entering the specificity pocket of trypsin (SP). N29 and R122 of PRSS1 are commonly mutated in hereditary pancreatitis (illustration provided by Andrew Brunskill PhD).
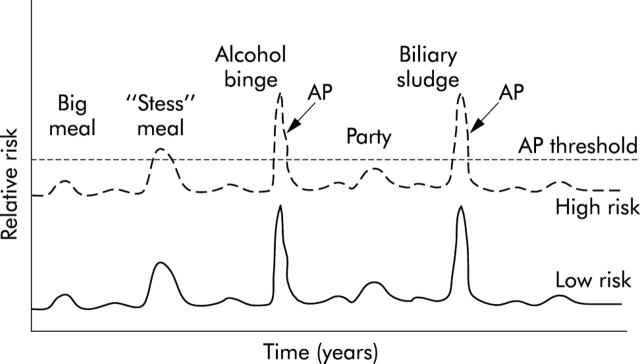
Susceptibility to acute pancreatitis (AP). Hypothetical relationship between pancreatitis risk factors and developing episodes of acute pancreatitis. Two subjects are illustrated who have identical environmental exposures but few genetic risk factors (low risk, bottom line) or significant risk factors (high risk, top line). The risk of developing pancreatitis at any point in time is likely variable, and reflects the combination of susceptibility factors and triggering factors that alter risk (for example, meals, alcohol, biliary, etc). Acute pancreatitis develops when the protective mechanisms are no longer adequate and the combined genetic and environmental risk factors and environmental triggers drive the pancreas over the threshold needed to initiate acute pancreatitis (AP threshold, broken line). Note that the subject with the higher underlying risk develops clinically recognised acute pancreatitis after several triggering events whereas the low risk subject does not develop acute pancreatitis with the same events.
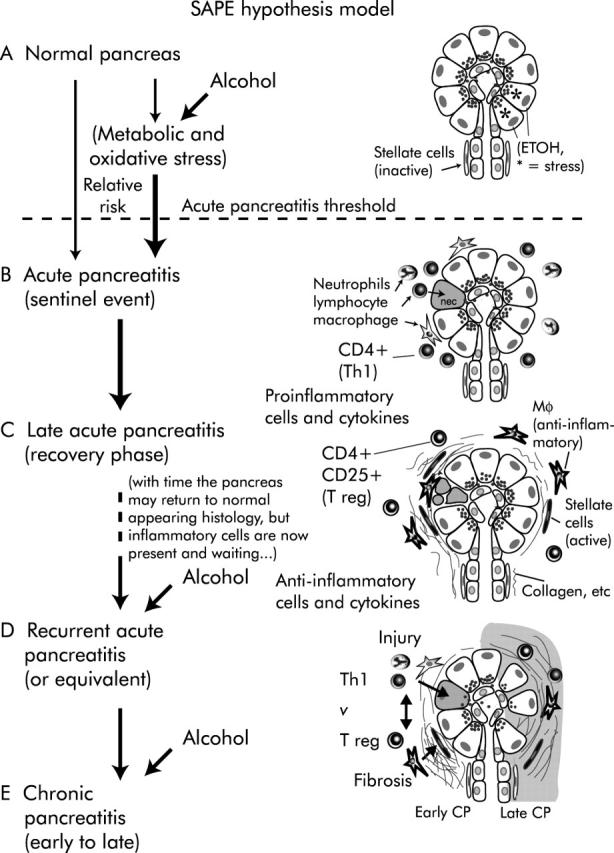
SAPE (sentinel acute pancreatitis event) hypothesis model. The sequence of events leading to chronic pancreatitis in the SAPE hypothesis model. (A) Normal pancreas. If the subject is a heavy alcohol user, acinar cells are under metabolic and oxidative stress (*) but histology remains relatively normal. Alcohol increases the risk of crossing the acute pancreatitis threshold (bold arrow crossing the broken line). (B) Acute pancreatitis with pancreatic injury and infiltration of proinflammatory cells. The first or “sentinel” acute pancreatitis event (SAPE) is a critical step because it initiates the inflammatory process that results in both injury and later fibrosis. (C) Late acute pancreatitis is dominated by anti-inflammatory cells that limit further injury by proinflammatory cells and products, and promote healing. This includes activation of stellate cells with produce collagen, etc. In the absence of recurrent acute pancreatitis, acinar cell toxins (for example, high dose alcohol), or factors that activate the immune system, the pancreas may eventually return to normal appearing histology except for some residual inflammatory cells that are primed to respond to any future injury. (D) Recurrent acute pancreatitis, acinar cell injury, or other factors that activate an acute inflammatory response (Th1) are immediately countered by an anti-inflammatory counter response (T reg) which, among other things, drives fibrosis. This vicious cycle results in both continued injury (top) and further fibrosis (bottom) leading to (E) extensive acinar cell loss and sclerosis (right) that is characteristic of chronic pancreatitis. Both genetic factors and environmental factors play a role in this process by increasing susceptibility to acute pancreatitis, altering the severity and duration of acute pancreatitis, and altering the healing processes that drive fibrosis. Alcohol is especially important because it acts at multiple steps in this process.
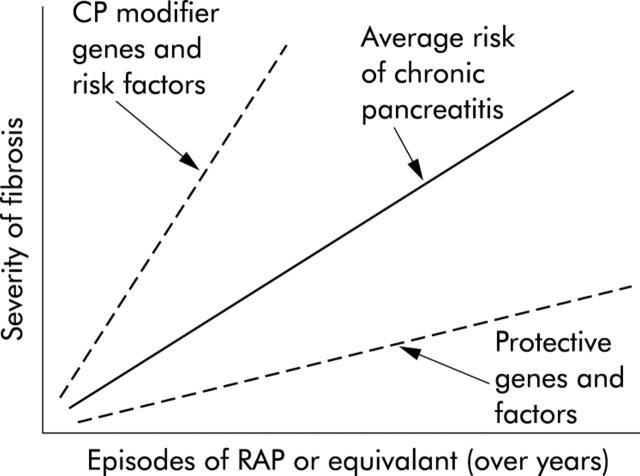
Modifier genes and factors effecting chronic pancreatitis. Hypothetical model illustrating the relationship between recurrent acute pancreatitis (RAP) or other immune system activating events (x axis) and the development of pancreatic fibrosis (y axis) which serves as a marker of severity of chronic pancreatitis. According to the SAPE hypothesis model, recurrent episodes of acute pancreatitis will lead to pancreatic fibrosis (average risk—solid line). Subjects with polymorphisms in modifier genes or who have other risk factors (chronic pancreatitis (CP) modifier genes—upper broken line) develop more fibrosis with less RAP, while patients with protective genes and factors (lower broken line) develop minimal fibrosis despite frequent RAP.
References
-
- Burke W . Genetic testing. N Engl J Med 2002;347:1867–75. - PubMed
-
- Applebaum SE, Kant JA, Whitcomb DC, et al. Genetic testing: counseling, laboratory and regulatory issues and the EUROPAC protocol for ethical research in multi-center studies of inherited pancreatic diseases. Med Clin North Am 2000;82:575–88. - PubMed
-
- Applebaum SE, O’Connell JA, Aston CE, et al. Motivations and concerns of patients with access to genetic testing for hereditary pancreatitis. Am J Gastroenterol 2001;96:1610–17. - PubMed
-
- Shaheen NJ, Lawrence LB, Bacon BR, et al. Insurance, employment, and psychosocial consequences of a diagnosis of hereditary hemochromatosis in subjects without end organ damage. Am J Gastroenterol 2003;98:1175–80. - PubMed
-
- Whitcomb DC. Early trypsinogen activation in acute pancreatitis. Gastroenterology 1999;116:770–3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical