

Use of alemtuzumab and tacrolimus monotherapy for cadaveric liver transplantation: with particular reference to hepatitis C virus
- PMID: 15480160
- PMCID: PMC2993510
- DOI: 10.1097/01.tp.0000142674.78268.01
Use of alemtuzumab and tacrolimus monotherapy for cadaveric liver transplantation: with particular reference to hepatitis C virus
Abstract
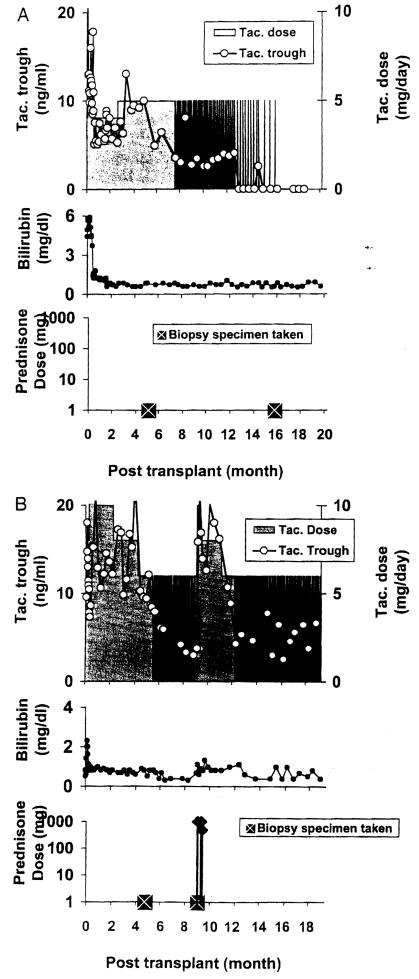
We have proposed that the mechanisms of alloengraftment and variable acquired tolerance can be facilitated by minimum posttransplant immunosuppression. It was further suggested that the efficacy of minimalistic treatment could be enhanced by preoperative recipient conditioning with an antilymphoid antibody preparation. A total of 76 adults (38 hepatitis C virus [HCV], 38 HCV) were infused with 30 mg alemtuzumab before primary cadaveric liver transplantation and maintained afterward on daily monotherapy unless breakthrough rejection mandated additional agents. In stable patients, the intervals between tacrolimus doses were lengthened ("spaced weaning") after approximately 4 months. Eighty-four contemporaneous nonlymphoid-depleted liver recipients (58 HCV, 26 HCV) were treated with conventional postoperative immunosuppression. The overall incidence of rejection was similar with the two strategies of immunosuppression. With follow-ups of 14 to 22 months, patient and primary graft survival in HCV cases are 97% and 90%, respectively, with alemtuzumab depletion plus minimal immunosuppression versus 71% and 70%, respectively, under conventional immunosuppression. In HCV recipients, current patient and graft survival in the alemtuzumab-pretreated group are 71% and 70% versus 65% and 54%, respectively, under conventional treatment. With both strategies of immunosuppression, the adverse effect of preexisting HCV on survival parameters and graft function already was significant at the 1-year milestone, but its extent was not evident until the second year. With or without HCV, 62% of the 64 surviving lymphoid-depleted patients are on spaced immunosuppression, and four patients receive no immunosuppression. Lymphoid depletion with alemtuzumab and minimalistic maintenance immunosuppression is a practical strategy of liver transplantation in HCV recipients but not HCV recipients.
Figures


Comment in
-
Prope tolerance with alemtuzumab.Liver Transpl. 2005 Mar;11(3):361-3. doi: 10.1002/lt.20366. Liver Transpl. 2005. PMID: 15719401 No abstract available.
References
-
- Hale G, Waldmann H, Dyer M. Specificity of monoclonal antibody Campath-1. Bone Marrow Transplant. 1988;3:237–239. - PubMed
-
- Calne R, Friend P, Moffatt S, et al. Prope tolerance, perioperative Campath 1H, and low-dose cyclosporin monotherapy in renal allograft recipients. Lancet. 1998;351:1701–1702. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
