

Balloon kyphoplasty for the treatment of pathological vertebral compressive fractures
- PMID: 15480827
- PMCID: PMC3476745
- DOI: 10.1007/s00586-004-0767-4
Balloon kyphoplasty for the treatment of pathological vertebral compressive fractures
Abstract
Background: Previous clinical studies have shown the safety and effectiveness of balloon kyphoplasty in the treatment of pathological vertebral compression fractures (VCFs). However, they have not dealt with the impact of relatively common comorbid conditions in this age group, such as spinal stenosis, and they have not explicitly addressed the use of imaging as a prognostic indicator for the restoration of vertebral body height. Neither have these studies dealt with management and technical problems related to surgery, nor the effectiveness of bone biopsy during the same surgical procedure. This is a prospective study comparing preoperative and postoperative vertebral body heights, kyphotic deformities, pain intensity (using visual analogue scale) and quality of life (Oswestry disability questionnaire) in patients with osteoporotic vertebral compression fractures (OVCFs) and osteolytic vertebral tumors treated with balloon kyphoplasty.
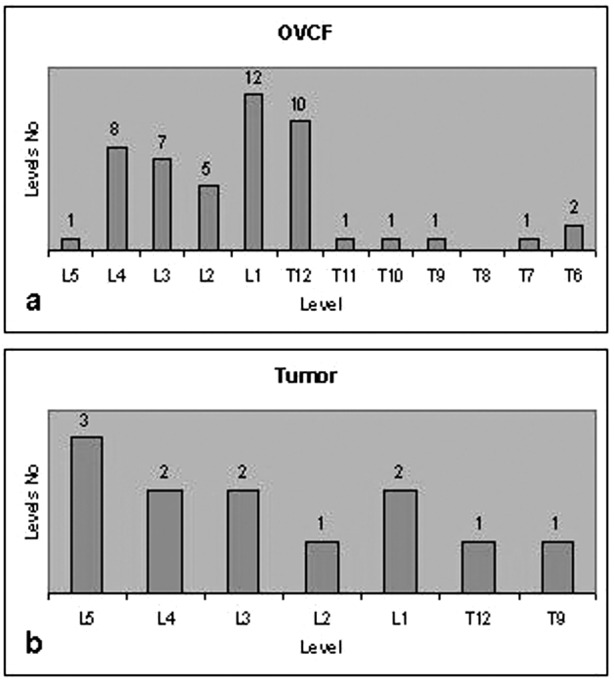
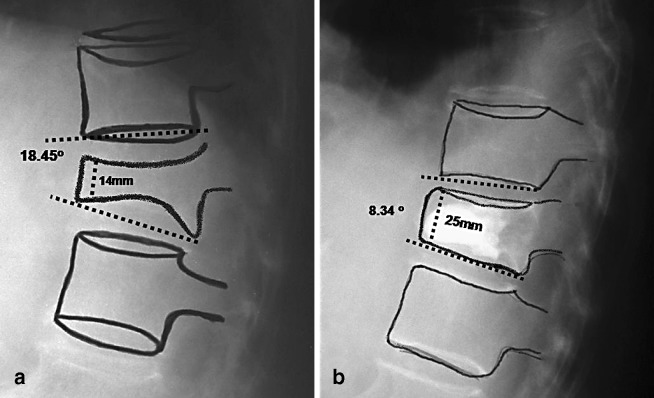
Methods: Thirty-two consecutive patients, 27 OVCFs (49 vertebral bodies [VBs]) and 5 patients suffering from VB tumor (12 VBs) were treated by balloon kyphoplasty. The mean age was 68.2 years. All patients were assessed within the first week of surgery, and then followed up after one, three and six months; all patients (27 OVCFs and 5 tumor patients) were followed up for 12 months, 17 patients (14 OVCFs and 3 tumors) were followed up for 18 months and 9 patients (8 OVCFs and 1 tumor) were followed up for 24 months (mean follow up 18 months). The correction of kyphosis and vertebral heights were measured by comparing preoperative and postoperative radiographic measurements.
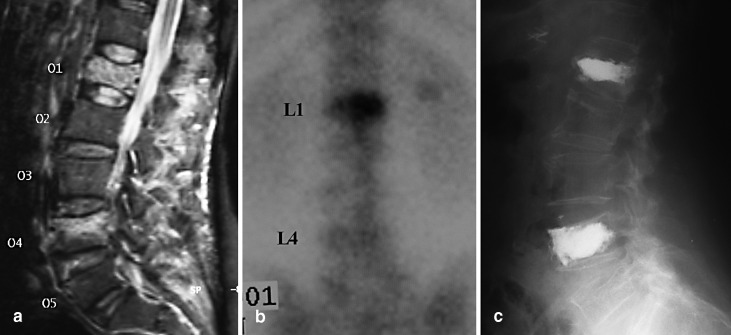
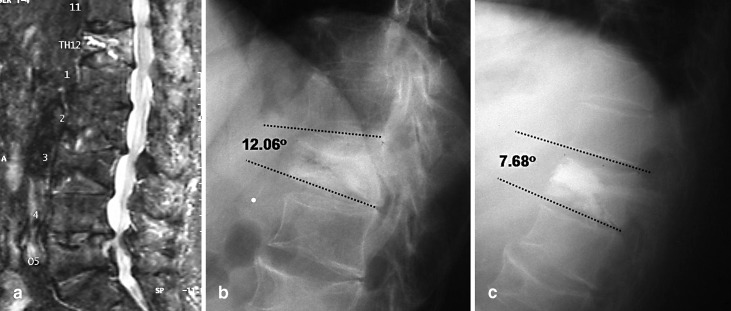
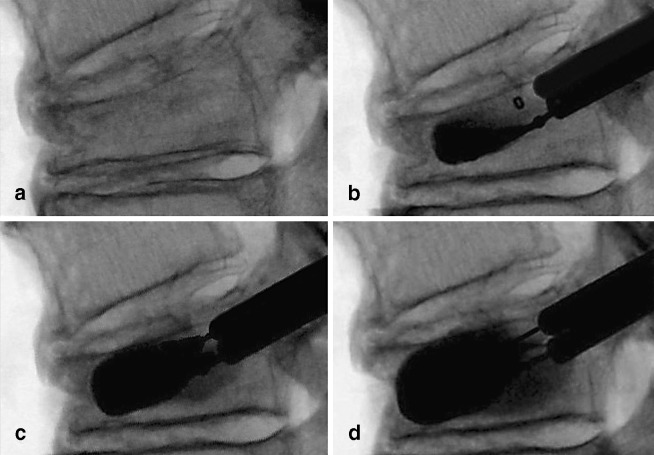
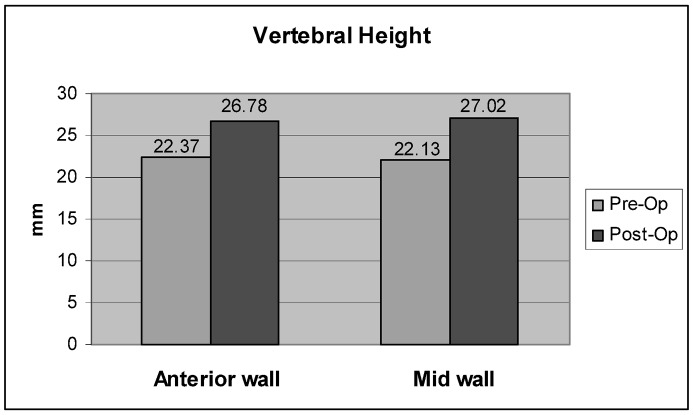
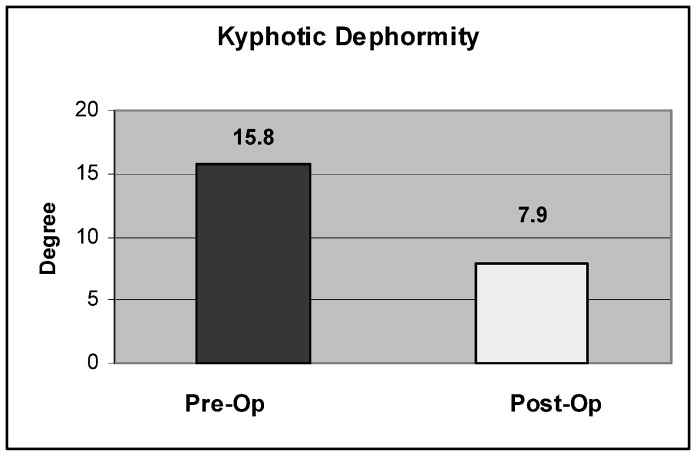
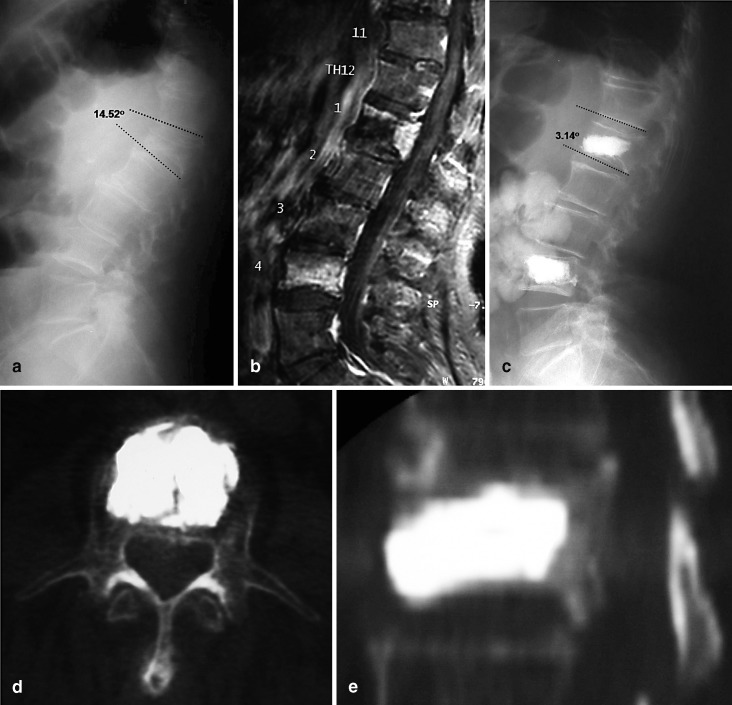
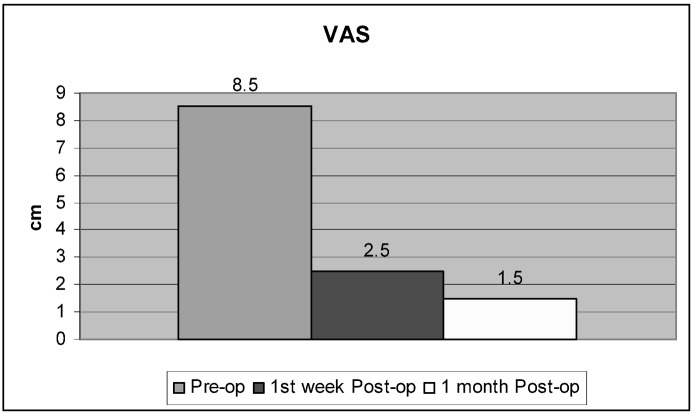
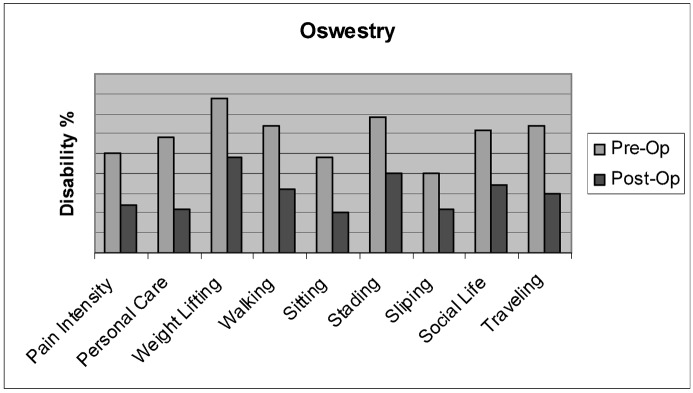
Results: Thirty-one patients (96.9%) exhibited significant and immediate pain improvement: 90% responded within 24 h and 6.3% responded within 5 days. Daily activities improved by 53% on the Oswestry scale. In the OVCF group, kyphosis correction was achieved in 24/27 patients (89.6%) with a mean correction of 7.6 degrees . Anterior wall height was restored in 43/49 VBs (88%) (mean increment of 4.3 mm), and mid vertebral body height was restored in 45/49 VBs (92%) (mean increment of 4.8 mm). Edema (high intensity signal) on short tau inversion recovery (STIR) was evidenced in all OVCF patients who experienced symptoms for less than nine months and was associated with correction of deformity. Cement leakage was the only technical problem encountered; it occurred in 5/49 VBs (10.2%) of the osteoporotic group and 1/12 VBs (8.3%) of the tumor group but had no clinical consequences. The incidence of leakage to the anterior epidural space was 2%. Spinal stenosis was present in three patients (11.1%) who responded successfully to subsequent laminectomy. Retrieval of tissue samples for biopsy was successful in 10/15 cases (67%). New fractures occurred in the adjacent level in 2/27 OVCF patients (7.4%).
Conclusions: Associated spinal stenosis with OVCF should not be overlooked; STIR MRI is a good predictor of deformity correction with balloon kyphoplasty. The prevalence of a new OVCF in the adjacent level is low.
Figures
Comment in
-
Reviewer's comment on: balloon kyphoplasty for the treatment of pathological vertebral compressive fractures (I.N. Gaitanis et al.).Eur Spine J. 2005 Apr;14(3):261-2. doi: 10.1007/s00586-004-0790-5. Eur Spine J. 2005. PMID: 15378416 Free PMC article. No abstract available.
-
The Michel Benoist and Robert Mulholland yearly European Spine Journal review: a survey of the "surgical and research" articles in the European Spine Journal, 2005.Eur Spine J. 2006 Jan;15(1):8-15. doi: 10.1007/s00586-005-1062-8. Epub 2006 Jan 13. Eur Spine J. 2006. PMID: 16411129 Free PMC article. Review. No abstract available.
-
The Michel Benoist and Robert Mulholland yearly European Spine Journal Review: a survey of the "medical" articles in the European Spine Journal, 2005.Eur Spine J. 2006 Jan;15(1):2-7. doi: 10.1007/s00586-005-1061-9. Epub 2006 Jan 13. Eur Spine J. 2006. PMID: 16411130 Free PMC article. Review. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
